

Cholecalciferol (vitamin D3) therapy and vitamin D insufficiency in patients with chronic kidney disease: a randomized controlled pilot study
- PMID: 18238736
- PMCID: PMC2654595
- DOI: 10.4158/EP.14.1.10
Cholecalciferol (vitamin D3) therapy and vitamin D insufficiency in patients with chronic kidney disease: a randomized controlled pilot study
Abstract
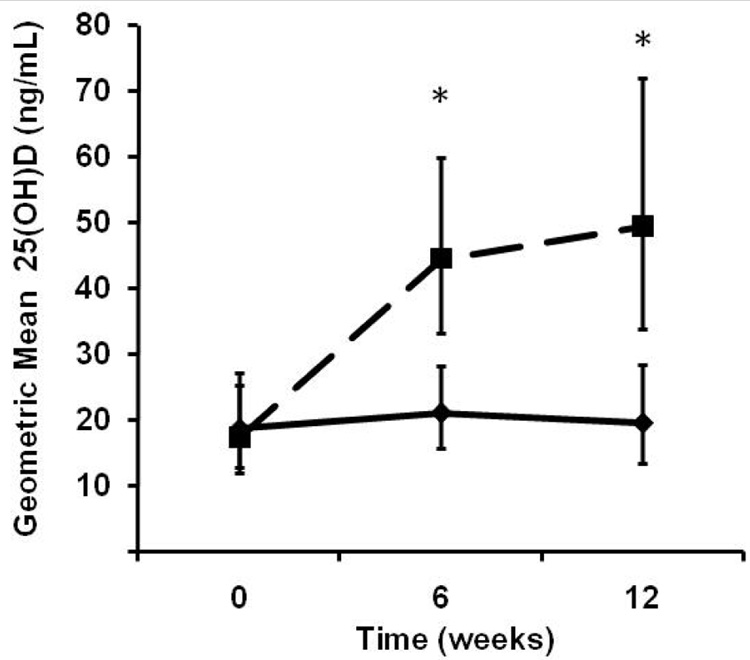
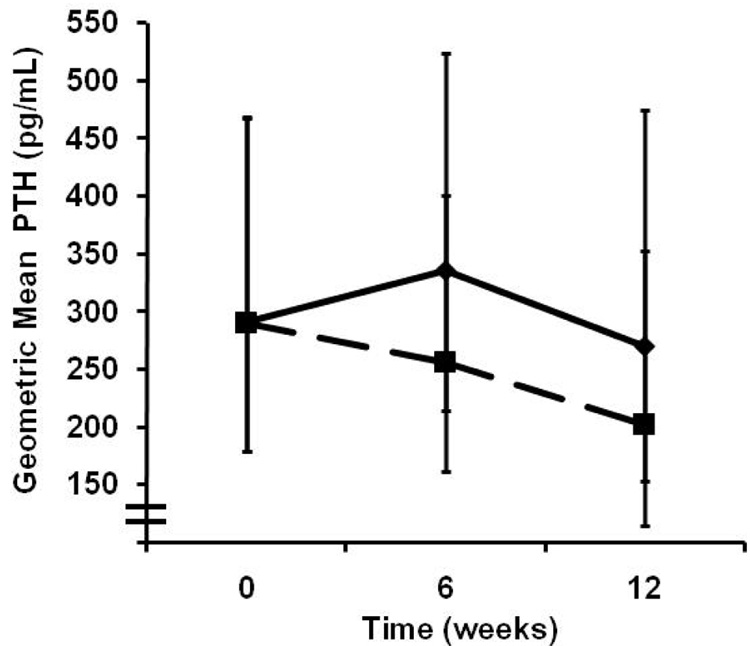
Objective: To investigate the efficacy of cholecalciferol (vitamin D3) in raising serum 25-hydroxyvitamin D (25[OH)]D) levels and reducing parathyroid hormone (PTH) levels in patients with chronic kidney disease (CKD).
Methods: In this double-blind, randomized controlled pilot study, participants with CKD stage 3 and 4 (estimated glomerular filtration rate, 15-59 mL/min/1.73 m2), vitamin D insufficiency (serum 25[OH]D <30 ng/mL), and serum intact PTH levels >70 pg/mL were randomly assigned to receive either 50 000 IU of cholecalciferol or placebo once weekly for 12 weeks. Primary outcomes (25[OH]D and PTH levels) were measured at baseline, week 6, and week 12. Secondary outcomes (1,25-dihydroxvitamin D and bone turnover markers) were measured at baseline and week 12. Because of skewed data distribution, statistical analyses were performed on a logarithmic scale. The difference between the group means was exponentiated to provide the geometric mean ratio. A linear mixed model using an unstructured variance-covariance matrix was used to examine change in the primary and secondary outcomes over time.
Results: Geometric mean serum 25(OH)D concentrations of the study groups were similar at baseline (P = .77). At week 6, a significant difference between the treatment and placebo groups was detected (P = .001); this difference was maintained at week 12 (P = .002). Among cholecalciferol-treated participants, serum 25(OH)D concentration increased on average from 17.3 ng/mL (95% confidence interval [CI], 11.8-25.2) at baseline to 49.4 ng/mL (95% CI, 33.9-72.0) at week 12. As-treated analysis indicated a trend toward lower PTH levels among cholecalciferol-treated participants (P = .07).
Conclusion: Weekly cholecalciferol supplementation appears to be an effective treatment to correct vitamin D status in patients with CKD.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
Similar articles
-
High-dose cholecalciferol reduces parathyroid hormone in patients with early chronic kidney disease: a pilot, randomized, double-blind, placebo-controlled trial.Am J Clin Nutr. 2012 Sep;96(3):672-9. doi: 10.3945/ajcn.112.040642. Epub 2012 Aug 1. Am J Clin Nutr. 2012. PMID: 22854402 Free PMC article. Clinical Trial.
-
Cholecalciferol v. ergocalciferol for 25-hydroxyvitamin D (25(OH)D) repletion in chronic kidney disease: a randomised clinical trial.Br J Nutr. 2016 Dec;116(12):2074-2081. doi: 10.1017/S000711451600427X. Epub 2017 Jan 9. Br J Nutr. 2016. PMID: 28065190 Free PMC article. Clinical Trial.
-
Cholecalciferol Supplementation Promotes Bone Turnover in Chinese Adults with Vitamin D Deficiency.J Nutr. 2018 May 1;148(5):746-751. doi: 10.1093/jn/nxy032. J Nutr. 2018. PMID: 29897564 Clinical Trial.
-
The Effect of Long-Term Cholecalciferol Supplementation on Vascular Calcification in Chronic Kidney Disease Patients With Hypovitaminosis D.J Ren Nutr. 2019 Sep;29(5):407-415. doi: 10.1053/j.jrn.2018.12.002. Epub 2019 Jan 25. J Ren Nutr. 2019. PMID: 30686750 Clinical Trial.
-
Efficacy and safety of a short course of very-high-dose cholecalciferol in hemodialysis.Am J Clin Nutr. 2012 Feb;95(2):522-8. doi: 10.3945/ajcn.111.025502. Epub 2012 Jan 11. Am J Clin Nutr. 2012. PMID: 22237061 Free PMC article. Clinical Trial.
Cited by
-
Bone Fragility in Chronic Kidney Disease Stage 3 to 5: The Use of Vitamin D Supplementation.Metabolites. 2022 Mar 20;12(3):266. doi: 10.3390/metabo12030266. Metabolites. 2022. PMID: 35323709 Free PMC article. Review.
-
Does Vitamin Supplementation Play a Role in Chronic Kidney Disease?Nutrients. 2023 Jun 23;15(13):2847. doi: 10.3390/nu15132847. Nutrients. 2023. PMID: 37447174 Free PMC article. Review.
-
Aiming Too Low: Reevaluation of Target Concentrations of Serum 25-Hydroxyvitamin D in Secondary Hyperparathyroidism.Am J Nephrol. 2019;49(4):281-283. doi: 10.1159/000499160. Epub 2019 Mar 15. Am J Nephrol. 2019. PMID: 30879016 Free PMC article. No abstract available.
-
Calcitriol Suppression of Parathyroid Hormone Fails to Improve Skeletal Properties in an Animal Model of Chronic Kidney Disease.Am J Nephrol. 2016;43(1):20-31. doi: 10.1159/000444423. Epub 2016 Feb 17. Am J Nephrol. 2016. PMID: 26881752 Free PMC article.
-
High doses of cholecalciferol alleviate the progression of hyperparathyroidism in patients with CKD Stages 3-4: results of a 12-week double-blind, randomized, controlled study.Nephrol Dial Transplant. 2018 Mar 1;33(3):466-471. doi: 10.1093/ndt/gfx059. Nephrol Dial Transplant. 2018. PMID: 29156056 Free PMC article. Clinical Trial.
References
-
- Holick MF. Sunlight and vitamin D for bone health and prevention of autoimmune diseases, cancers, and cardiovascular disease. Am J Clin Nutr. 2004;80 Suppl 6:1678–1688. - PubMed
-
- Heaney RP. The Vitamin D requirement in health and disease. J Steroid Biochem Mol Biol. 2005;97:13–19. - PubMed
-
- DeLuca HF. Overview of general physiologic features and functions of vitamin D. Am J Clin Nutr. 2004;80 Suppl 6:1689–1696. - PubMed
-
- Lips P. Vitamin D deficiency and secondary hyperparathyroidism in the elderly: consequences for bone loss and fractures and therapeutic implications. Endocr Rev. 2001;22:477–501. - PubMed
-
- Slatopolsky E, Brown A, Dusso A. Pathogenesis of secondary hyperparathyroidism. Kidney Int Suppl. 1999;73:14–19. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
