

Assessment of gastrointestinal stromal tumors with computed tomography following treatment with imatinib mesylate
- PMID: 18240346
- PMCID: PMC2687056
- DOI: 10.3748/wjg.14.892
Assessment of gastrointestinal stromal tumors with computed tomography following treatment with imatinib mesylate
Abstract
Aim: To evaluate and characterize the patterns of disease progression of metastatic or unresectable gastrointestinal stromal tumor (GIST) treated with imatinib mesylate, and to determine the prognostic significance associated with disease progression.
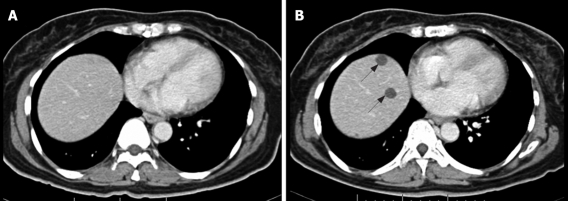
Methods: Clinical data and computed tomography (CT) images were retrospectively reviewed in 17 GIST patients who were treated with imatinib mesylate from October 2002 to October 2006. Apart from using size measurement for evaluation of tumor response [Response Evaluation Criteria in Solid Tumors (RECIST) criteria], patterns of CT changes during treatment were evaluated and correlated with clinical data.
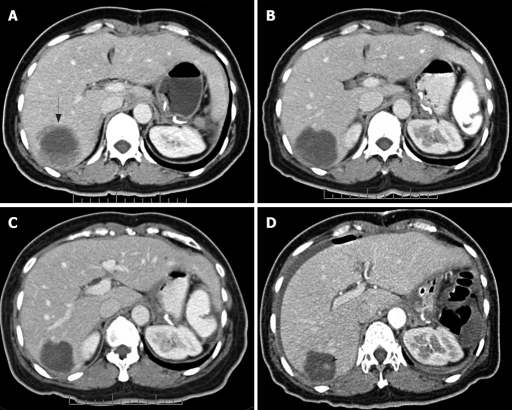
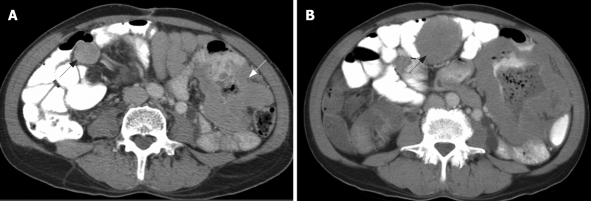
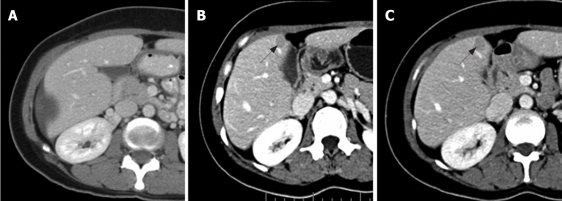
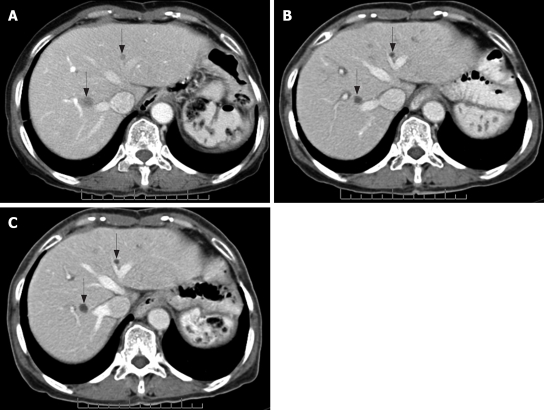
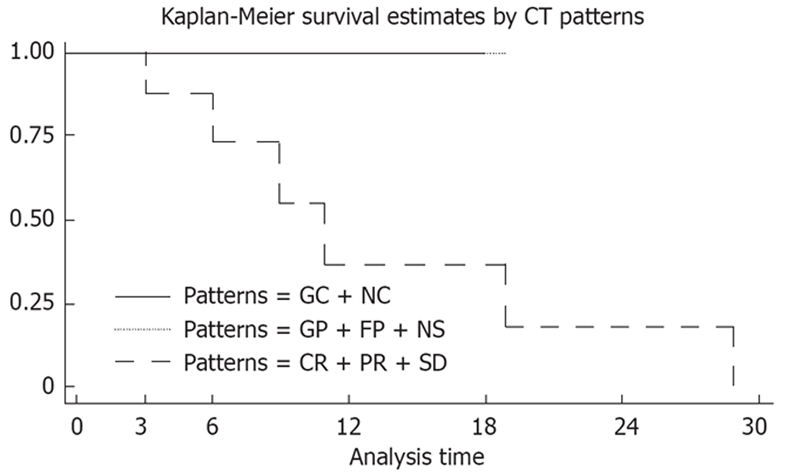
Results: There were eight non-responders and nine responders. Five patterns of CT change during treatment were found: focal progression (FP), generalized progression (GP), generalized cystic change (GC), new cystic lesion (NC) and new solid lesion (NS). At the end of study, all non-responders showed GP, whereas responders showed cystic change (GC and NC) and response according to RECIST criteria. Overall survival was significantly better in patients with cystic change or response within the RECIST criteria compared with GP patients (P = 0.0271).
Conclusion: Various patterns of CT change in patients with GIST who responded to imatinib mesylate were demonstrated, and might determine the prognosis of the disease. A combination of RECIST criteria and pattern of CT change are proposed for response evaluation in GIST.
Figures
References
-
- Horton KM, Fishman EK. Current role of CT in imaging of the stomach. Radiographics. 2003;23:75–87. - PubMed
-
- Burkill GJ, Badran M, Al-Muderis O, Meirion Thomas J, Judson IR, Fisher C, Moskovic EC. Malignant gastrointestinal stromal tumor: distribution, imaging features, and pattern of metastatic spread. Radiology. 2003;226:527–532. - PubMed
-
- Lau S, Tam KF, Kam CK, Lui CY, Siu CW, Lam HS, Mak KL. Imaging of gastrointestinal stromal tumour (GIST) Clin Radiol. 2004;59:487–498. - PubMed
-
- Stroszczynski C, Jost D, Reichardt P, Chmelik P, Gaffke G, Kretzschmar A, Schneider U, Felix R, Hohenberger P. Follow-up of gastro-intestinal stromal tumours (GIST) during treatment with imatinib mesylate by abdominal MRI. Eur Radiol. 2005;15:2448–2456. - PubMed
-
- Joensuu H, Fletcher C, Dimitrijevic S, Silberman S, Roberts P, Demetri G. Management of malignant gastrointestinal stromal tumours. Lancet Oncol. 2002;3:655–664. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
