

Posterior compartment anatomy as seen in magnetic resonance imaging and 3-dimensional reconstruction from asymptomatic nulliparas
- PMID: 18241813
- PMCID: PMC2876342
- DOI: 10.1016/j.ajog.2007.11.032
Posterior compartment anatomy as seen in magnetic resonance imaging and 3-dimensional reconstruction from asymptomatic nulliparas
Abstract
Objective: The objective of the study was to identify characteristic anatomical features of the posterior compartment using magnetic resonance (MR) cross-sectional anatomy and 3-dimensional (3-D) modeling.
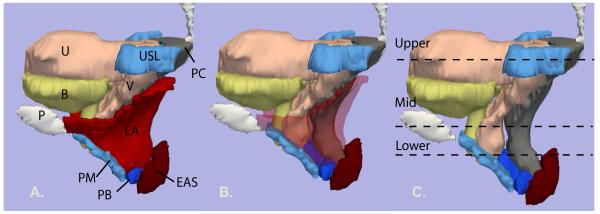
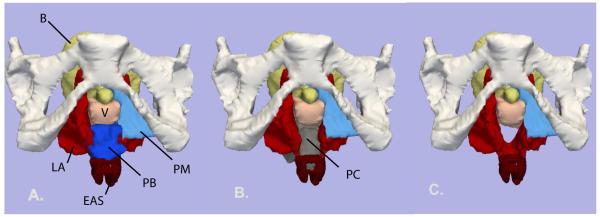
Study design: Supine, static proton-density MR images of 20 nulliparas were analyzed. MR images were used to create models in a selected exemplar.
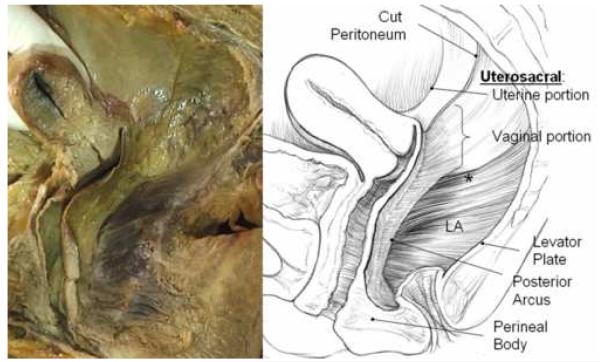
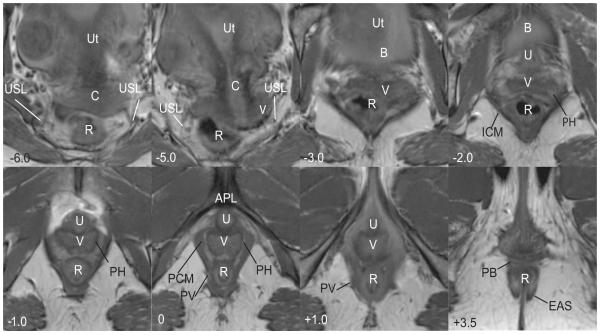
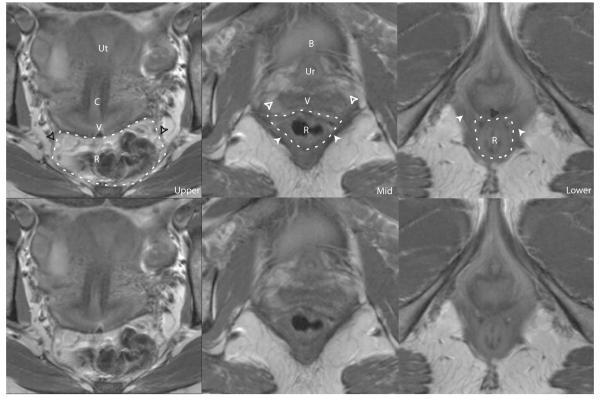
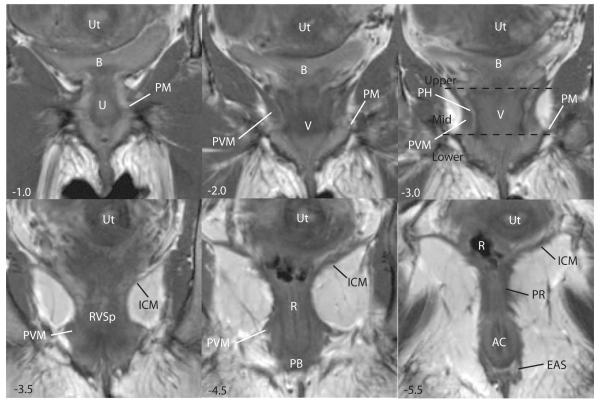
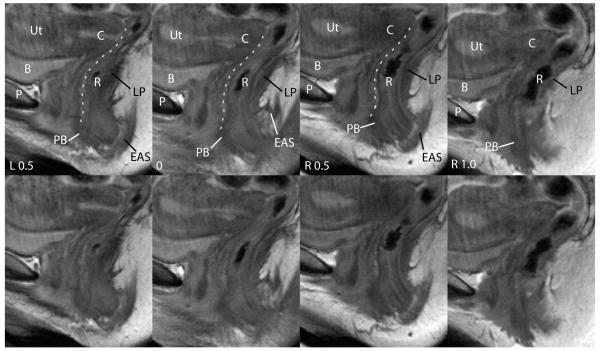
Results: The compartment's upper, mid, and lower segments are best seen in the axial plane. It is bounded inferiorly by the perineal body, ventrally by the posterior vaginal wall, and dorsally by the levator ani muscles and coccyx. In the upper portion, the compartment is bordered laterally by the uterosacral ligaments, whereas in the middle portion, there is more direct contact with the lateral levator ani muscles. In the lower portion, the contact becomes obliterated because the vagina and levator ani muscles become fused to each another and to the perineal body.
Conclusion: The posterior compartment has characteristic anatomic features in MR cross-sectional anatomy that can be further elucidated and integrated with 3-D anatomy.
Figures
References
-
- Boyles SH, Weber AM, Meyn L. Procedures for pelvic organ prolapse in the united states, 1979-1997. Am J Obstet Gynecol. 2003;188(1):108–15. - PubMed
-
- Silva WA, Pauls RN, Segal JL, Rooney CM, Kleeman SD, Karram MM. Uterosacral ligament vault suspension: Five-year outcomes. Obstet Gynecol. 2006;108(2):255–63. - PubMed
-
- DeLancey JO. Anatomic aspects of vaginal eversion after hysterectomy. Am J Obstet Gynecol. 1992;166:1717–1728. - PubMed
-
- Leffler KS, Thompson JR, Cundiff GW, Buller JL, Burrows LJ, Ybarra MA Schon. Attachment of the rectovaginal septum to the pelvic sidewall. Am J Obstet Gynecol. 2001;185(1):41–3. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
