

Differentiating obstructive from central and complex sleep apnea using an automated electrocardiogram-based method
- PMID: 18246985
- PMCID: PMC2276128
- DOI: 10.1093/sleep/30.12.1756
Differentiating obstructive from central and complex sleep apnea using an automated electrocardiogram-based method
Abstract
Study objectives: Complex sleep apnea is defined as sleep disordered breathing secondary to simultaneous upper airway obstruction and respiratory control dysfunction. The objective of this study was to assess the utility of an electrocardiogram (ECG)-based cardiopulmonary coupling technique to distinguish obstructive from central or complex sleep apnea.
Design: Analysis of archived polysomnographic datasets.
Setting: A laboratory for computational signal analysis.
Interventions: None.
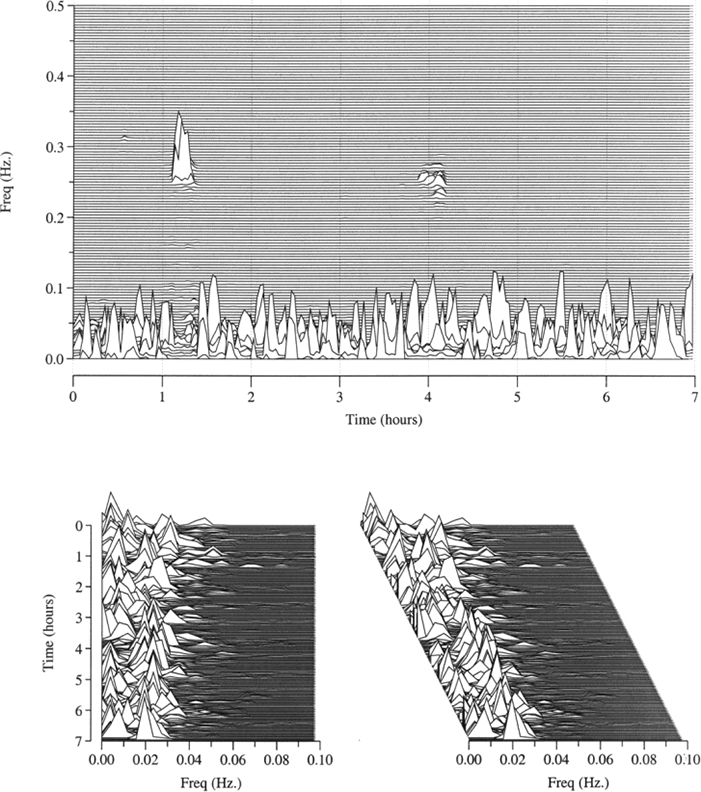
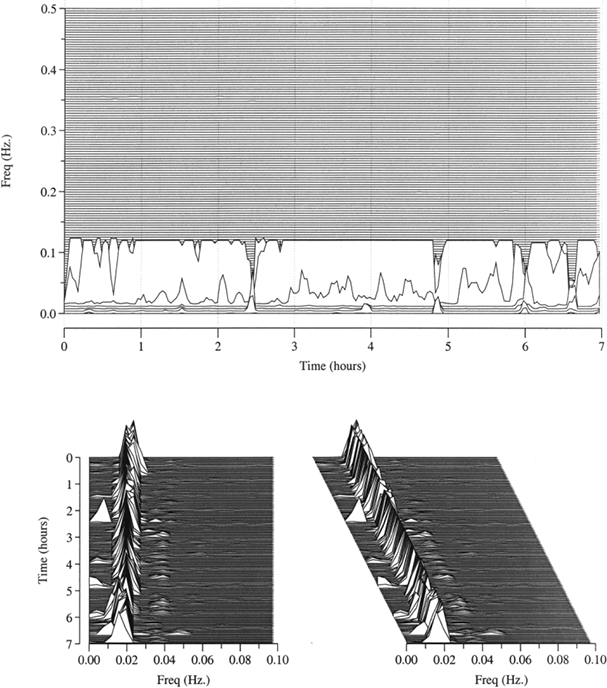
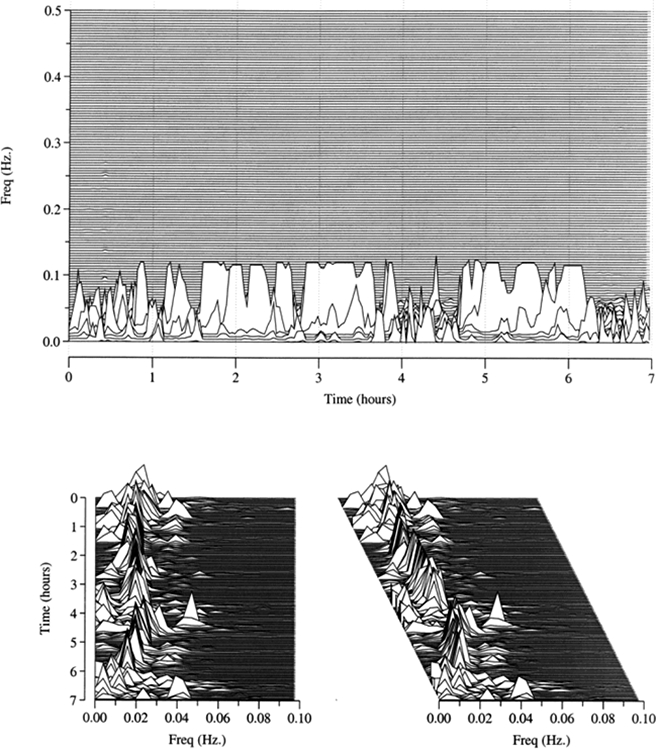
Measurements and results: The PhysioNet Sleep Apnea Database, consisting of 70 polysomnograms including single-lead ECG signals of approximately 8 hours duration, was used to train an ECG-based measure of autonomic and respiratory interactions (cardiopulmonary coupling) to detect periods of apnea and hypopnea, based on the presence of elevated low-frequency coupling (e-LFC). In the PhysioNet BIDMC Congestive Heart Failure Database (ECGs of 15 subjects), a pattern of "narrow spectral band" e-LFC was especially common. The algorithm was then applied to the Sleep Heart Health Study-I dataset, to select the 15 records with the highest amounts of broad and narrow spectral band e-LFC. The latter spectral characteristic seemed to detect not only periods of central apnea, but also obstructive hypopneas with a periodic breathing pattern. Applying the algorithm to 77 sleep laboratory split-night studies showed that the presence of narrow band e-LFC predicted an increased sensitivity to induction of central apneas by positive airway pressure.
Conclusions: ECG-based spectral analysis allows automated, operator-independent characterization of probable interactions between respiratory dyscontrol and upper airway anatomical obstruction. The clinical utility of spectrographic phenotyping, especially in predicting failure of positive airway pressure therapy, remains to be more thoroughly tested.
Figures

References
-
- Sleep-related breathing disorders in adults: recommendations for syndrome definition and measurement techniques in clinical research. The Report of an American Academy of Sleep Medicine Task Force. Sleep. 1999;22:667–89. - PubMed
-
- Hosselet JJ, Norman RG, Ayappa I, Rapoport DM. Detection of flow limitation with a nasal cannula/pressure transducer system. Am J Respir Crit Care Med. 1998;157:1461–7. - PubMed
-
- Badr MS. Central sleep apnea. Prim Care. 2005;32:361–74. - PubMed
-
- Onal E, Burrows DL, Hart RH, Lopata M. Induction of periodic breathing during sleep causes upper airway obstruction in humans. J Appl Physiol. 1986;61:1438–43. - PubMed
-
- Badr MS, Toiber F, Skatrud JB, Dempsey J. Pharyngeal narrowing/occlusion during central sleep apnea. J Appl Physiol. 1995;78:1806–15. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
