

Primary versus specialty care outcomes for depressed outpatients managed with measurement-based care: results from STAR*D
- PMID: 18247097
- PMCID: PMC2324144
- DOI: 10.1007/s11606-008-0522-3
Primary versus specialty care outcomes for depressed outpatients managed with measurement-based care: results from STAR*D
Abstract
Background: Whether the acute outcomes of major depressive disorder (MDD) treated in primary (PC) or specialty care (SC) settings are different is unknown.
Objective: To compare the treatment and outcomes for depressed outpatients treated in primary versus specialty settings with citalopram in the Sequenced Treatment Alternatives to Relieve Depression (STAR*D) study (www.star-d.org), a broadly inclusive effectiveness trial.
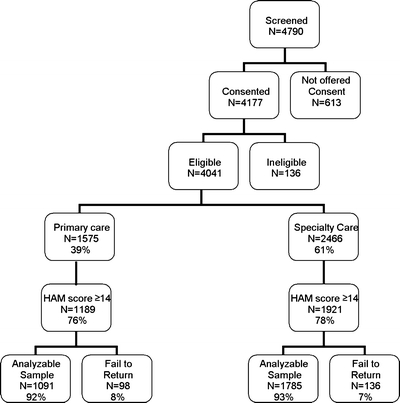
Design: Open clinical trial with citalopram for up to 14 weeks at 18 primary and 23 specialty sites. Participants received measurement-based care with 5 recommended treatment visits, manualized pharmacotherapy, ongoing support and guidance by a clinical research coordinator, the use of structured evaluation of depressive symptoms and side effects at each visit, and a centralized treatment monitoring and feedback system.
Participants: A total of 2,876 previously established outpatients in primary (n = 1091) or specialty (n = 1785) with nonpsychotic depression who had at least 1 post-baseline measure.
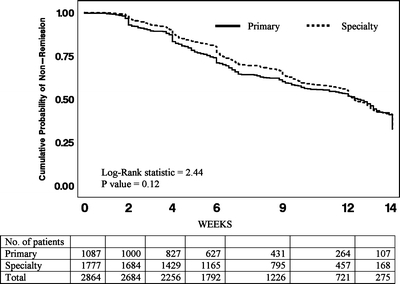
Measurements and main results: Remission (Hamilton Depression Rating Scale for Depression [Hamilton] or 16-item Quick Inventory of Depressive Symptomatology-Self-Rated [QIDS-SR(16)]); response (QIDS-SR(16)); time to first remission (QIDS-SR(16)). Remission rates by Hamilton (26.6% PC vs 28.0% SC, p = .40) and by QIDS-SR(16) (32.5% PC vs 33.1% SC, p = .78) and response rates by QIDS-SR(16) (45.7% PC vs 47.6% SC, p = .33) were not different. For those who reached remission or response at exit, the time to remission (6.2 weeks PC vs 6.9 weeks SC, p = .12) and to response (5.5 weeks PC vs 5.4 weeks SC, p = .97) did not differ by setting.
Conclusions: Identical remission and response rates can be achieved in primary and specialty settings when identical care is provided.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
