

Primary bone tumors of adulthood
- PMID: 18250012
- PMCID: PMC1434587
- DOI: 10.1102/1470-7330.2004.0004
Primary bone tumors of adulthood
Abstract
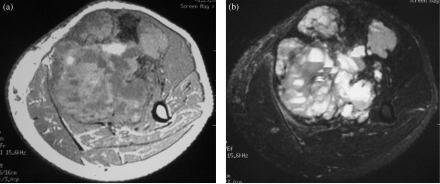
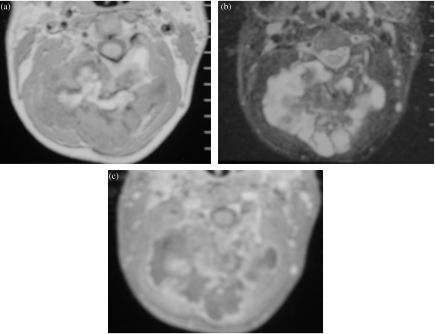
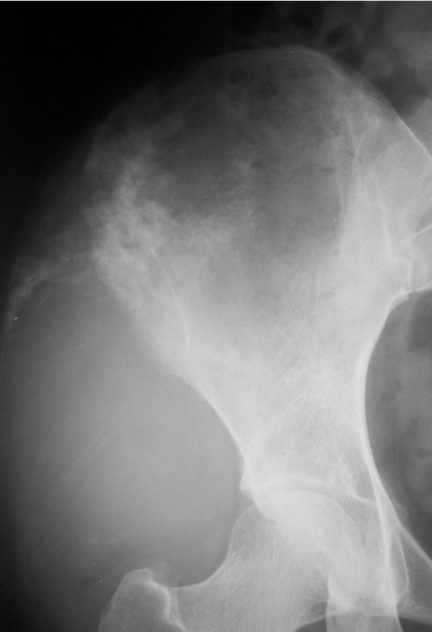
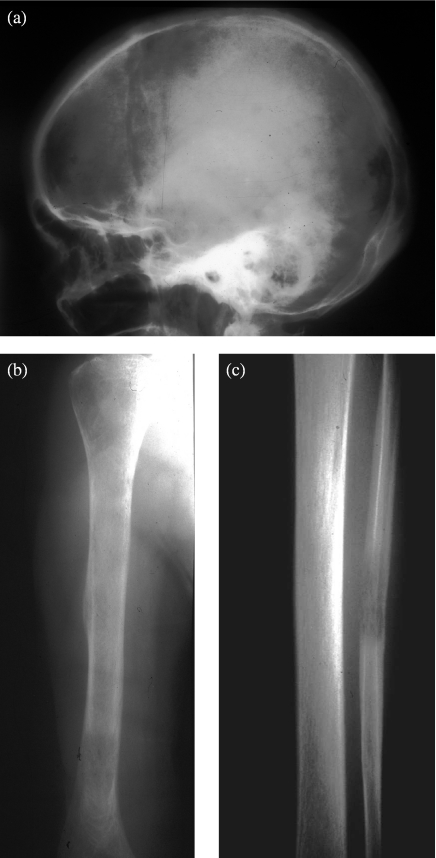
Imaging plays a crucial role in the evaluation of primary bone tumors in adults. Initial radiographic evaluation is indicated in all cases with suspected primary bone tumors. Radiographs are useful for providing the diagnosis, a short list of differential diagnosis or at least indicating the degree of aggressiveness of the lesion. More detailed information about the lesion, such as cortical destruction or local spread, can be obtained using cross-sectional imaging techniques such as computed tomography and magnetic resonance imaging. This article discusses the characteristic features of the more common primary bone tumors of adulthood, and also the pre-treatment evaluation and staging of these lesions using imaging techniques.
Figures






Similar articles
-
Imaging Features of Bone Tumors: Conventional Radiographs and MR Imaging Correlation.Magn Reson Imaging Clin N Am. 2019 Nov;27(4):753-767. doi: 10.1016/j.mric.2019.07.008. Magn Reson Imaging Clin N Am. 2019. PMID: 31575404 Review.
-
The current role of radiography in the assessment of skeletal tumors and tumor-like lesions.Eur J Radiol. 1998 May;27 Suppl 1:S77-85. doi: 10.1016/s0720-048x(98)00047-3. Eur J Radiol. 1998. PMID: 9652506 Review.
-
Clear cell chondrosarcoma: radiographic, computed tomographic, and magnetic resonance findings in 34 patients with pathologic correlation.Skeletal Radiol. 2003 Dec;32(12):687-94. doi: 10.1007/s00256-003-0668-3. Epub 2003 Oct 7. Skeletal Radiol. 2003. PMID: 14530882
-
Proceedings of the European Society of Musculoskeletal Radiology (ESSR) training module, Antwerp, 20-21.01.05. Part two: bone tumors. Benign bone lesions: characteristic imaging features.JBR-BTR. 2006 Sep-Oct;89(5):266-74. JBR-BTR. 2006. PMID: 17147017
-
More advantages in detecting bone and soft tissue metastases from prostate cancer using 18F-PSMA PET/CT.Hell J Nucl Med. 2019 Jan-Apr;22(1):6-9. doi: 10.1967/s002449910952. Epub 2019 Mar 7. Hell J Nucl Med. 2019. PMID: 30843003
Cited by
-
Bone tumors: state-of-the-art imaging.Skeletal Radiol. 2024 Sep;53(9):1783-1798. doi: 10.1007/s00256-024-04621-7. Epub 2024 Feb 27. Skeletal Radiol. 2024. PMID: 38409548 Review.
-
Impaction of Deciduous and Permanent Teeth Related to Local Obstacles: A Retrospective Study of 10 Years of Institutional Experience.Children (Basel). 2025 Jul 14;12(7):929. doi: 10.3390/children12070929. Children (Basel). 2025. PMID: 40723121 Free PMC article.
-
Fluorodeoxyglucose Positron Emission Tomography-Computed Tomography (FDG PET/CT) Findings in an Unusual Case of Multiple Myeloma Presenting with a Large Extra-Axial Intracranial Mass.Pol J Radiol. 2016 Dec 16;81:602-605. doi: 10.12659/PJR.899444. eCollection 2016. Pol J Radiol. 2016. PMID: 28058074 Free PMC article.
-
Clinical characteristic-assisted surgical benefit stratification for resection of primary tumor in patients with advanced primary malignant bone neoplasms: a population-based propensity score-matched analysis.Front Oncol. 2023 Sep 6;13:960502. doi: 10.3389/fonc.2023.960502. eCollection 2023. Front Oncol. 2023. PMID: 37746283 Free PMC article.
-
Trends in medicare reimbursement for the resection of spinal tumors: 2000-2021.Neurosurg Rev. 2025 Aug 19;48(1):611. doi: 10.1007/s10143-025-03742-4. Neurosurg Rev. 2025. PMID: 40828204 Free PMC article.
References
-
- Peh WC. The role of imaging in the staging of bone tumors. Crit Rev Oncol Hematol. 1999;31:147–67. - PubMed
-
- Lodwick GS, Wilson AJ, Farrell C, Virtama P, Dittrich F. Determining growth rates of focal lesions of bones from radiographs. Radiology. 1980;134:577–83. - PubMed
-
- Nomikos GC, Murphey MD, Kransdorf MJ, Bancroft LW, Peterson JJ. Primary bone tumors of the lower extremities. Radiol Clin North Am. 2002;40:971–90. - PubMed
-
- Resnick D, Greenway GD. Tumors and tumor-like lesions of bone: imaging and pathology of specific lesions. In: Resnick D, editor. Bone and Joint Imaging. 2nd edn. Philadelphia, PA: W.B. Saunders; 1996. pp. 991–1065.
-
- Spina V, Montanari N, Romagnoli R. Malignant tumors of the osteogenic matrix. Eur J Radiol. 1998;27(Suppl. 1):S98–109. - PubMed
LinkOut - more resources
Full Text Sources