

Endoscopic ultrasound in the detection of pancreatic islet cell tumours
- PMID: 18250013
- PMCID: PMC1434588
- DOI: 10.1102/1470-7330.2004.0008
Endoscopic ultrasound in the detection of pancreatic islet cell tumours
Abstract
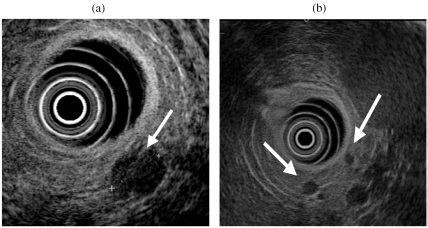
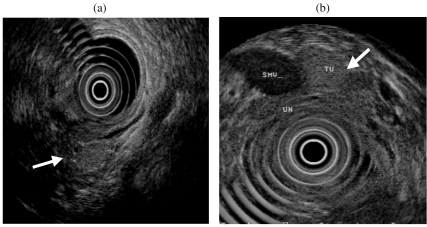
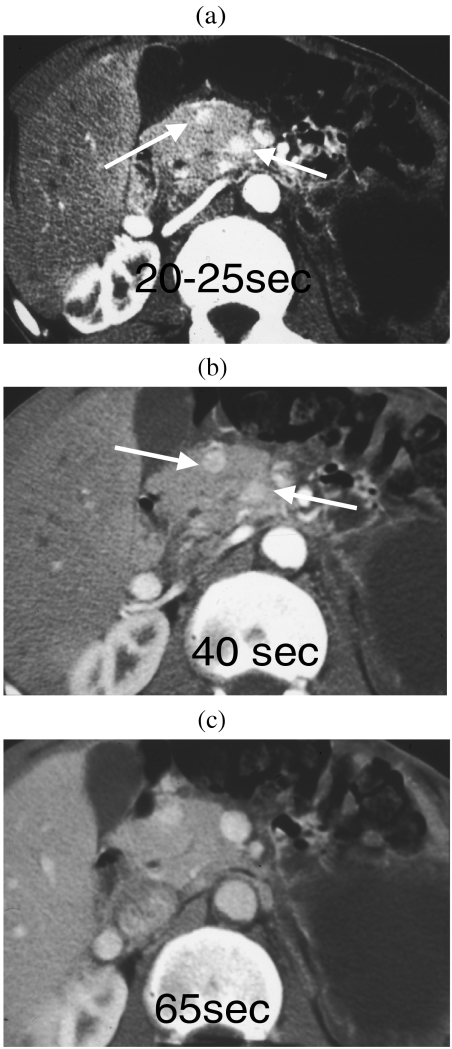
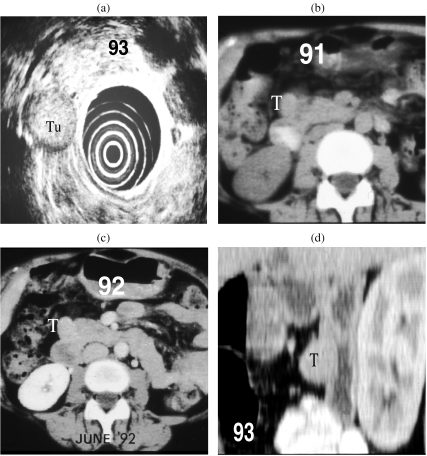
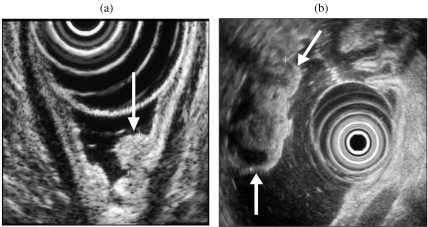
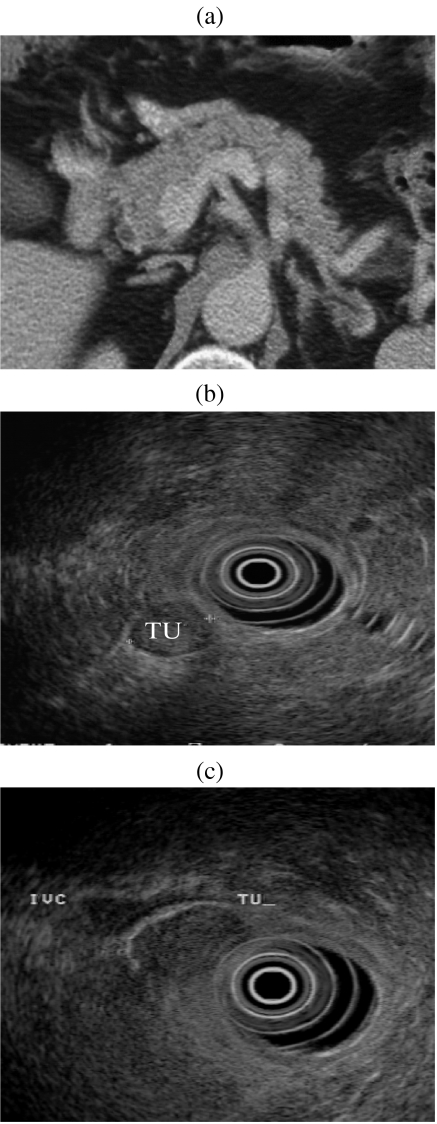
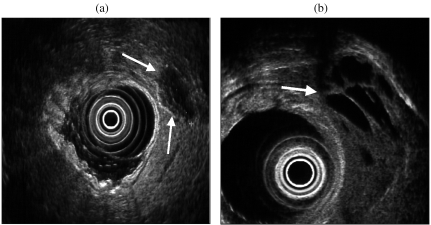
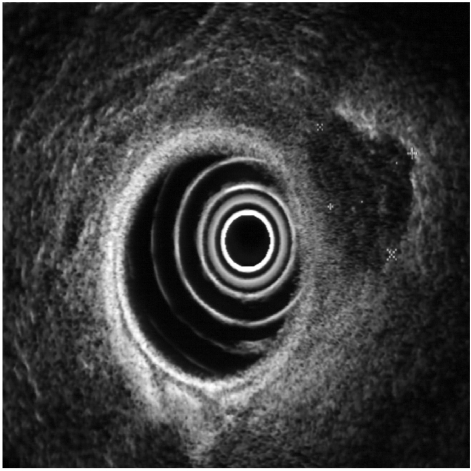
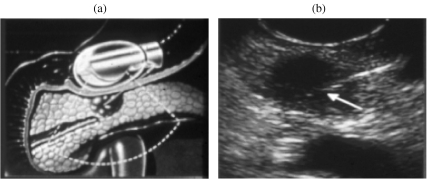
The role of endoscopic ultrasound (EUS) in the detection of pancreatic islet cell tumours is reviewed. Functioning islet cell tumours are frequently small at presentation (90%< 2 cm). Advances in cross-sectional imaging with CT and MRI have resulted in improved detection rates of these small lesions. The sensitivity of EUS in the detection of insulinoma is similar to helical or multislice CT, i.e. between 82 and 94%, while a combination of both techniques is reported to identify 100% of tumours. EUS may be considered a primary diagnostic tool in these patients. EUS has a secondary role in the detection of gastrinomas as over 50% are malignant and 5% extra-pancreatic in position. CT should be used as a first-line investigation. EUS is valuable in problem solving in these patients. EUS has a role in staging large tumours prior to surgery. EUS-guided fine needle aspiration may provide cytological confirmation of the nature of a tumour prior to surgery.
Figures

Similar articles
-
Endoscopic ultrasound-guided fine-needle aspiration biopsy (EUS-FNA) in insulinomas: Indications and clinical relevance in a single investigator cohort of 47 patients.Endocrine. 2017 Apr;56(1):158-163. doi: 10.1007/s12020-016-1179-z. Epub 2016 Nov 30. Endocrine. 2017. PMID: 27905047
-
Endoscopic ultrasound in the localisation of pancreatic islet cell tumours.Best Pract Res Clin Endocrinol Metab. 2005 Jun;19(2):177-93. doi: 10.1016/j.beem.2004.11.012. Best Pract Res Clin Endocrinol Metab. 2005. PMID: 15763694 Review.
-
Pancreatic cancer--EUS and early diagnosis.Langenbecks Arch Surg. 2008 Nov;393(6):923-7. doi: 10.1007/s00423-007-0275-1. Epub 2008 Feb 5. Langenbecks Arch Surg. 2008. PMID: 18247044 Review.
-
Pretherapeutic evaluation of patients with upper gastrointestinal tract cancer using endoscopic and laparoscopic ultrasonography.Dan Med J. 2012 Dec;59(12):B4568. Dan Med J. 2012. PMID: 23290296 Review.
-
Role of repeated endoscopic ultrasound-guided fine needle aspiration in small solid pancreatic masses with previous indeterminate and negative cytological findings.Dig Dis. 2008;26(4):377-82. doi: 10.1159/000177025. Epub 2009 Jan 30. Dig Dis. 2008. PMID: 19188731 Clinical Trial.
Cited by
-
Metastatic insulinoma in a patient with type 2 diabetes mellitus: case report and review of the literature.Int J Endocrinol. 2011;2011:124078. doi: 10.1155/2011/124078. Epub 2011 Feb 10. Int J Endocrinol. 2011. PMID: 21331288 Free PMC article.
-
Management of pancreatic neuroendocrine tumors in patients with MEN 1.Gland Surg. 2015 Feb;4(1):63-8. doi: 10.3978/j.issn.2227-684X.2014.12.01. Gland Surg. 2015. PMID: 25713781 Free PMC article. Review.
-
Endoscopic ultrasound-guided fine-needle aspiration biopsy (EUS-FNA) in insulinomas: Indications and clinical relevance in a single investigator cohort of 47 patients.Endocrine. 2017 Apr;56(1):158-163. doi: 10.1007/s12020-016-1179-z. Epub 2016 Nov 30. Endocrine. 2017. PMID: 27905047
-
The functioning side of the pancreas: a review on insulinomas.J Endocrinol Invest. 2020 Feb;43(2):139-148. doi: 10.1007/s40618-019-01091-w. Epub 2019 Jul 31. J Endocrinol Invest. 2020. PMID: 31368049 Review.
-
Role of (68)Ga-DOTATATE PET/CT in patients with multiple endocrine neoplasia type 1 (MEN1).Endocrine. 2016 Jun;52(3):488-94. doi: 10.1007/s12020-015-0702-y. Epub 2015 Aug 5. Endocrine. 2016. PMID: 26242621
References
-
- Phan GQ, Yeo CJ, Hruban RH, Lillemoe KD, Pitt HA, Cameron JL. Surgical experience with pancreatic and periancreatic neuroendocrine tumours: review of 125 patients. J Gastrointest Surg. 1998;2:472–82. - PubMed
-
- King CM, Reznek RH, Dacie JE, Wass JA. Imaging islet cell tumours. Clin Radiol. 1994;49:295–303. - PubMed
-
- Gunther RW, Klose KJ, Ruckert K, Beyer J, Kuhn FP, Klotter HJ. Localization of small islet-cell tumors. Preoperative and intra-operative ultrasound, computed tomography, arteriography, digital subtraction angiography, and pancreatic venous sampling. Gastrointest Radiol. 1985;10:145–52. - PubMed
-
- Rösch T, Lightdale CJ, Botet JF, et al. Localization of pancreatic endocrine tumors by endoscopic ultrasonography. N Engl J Med. 1992;326:1721–6. - PubMed
-
- Pitre J, Soubrane O, Palazzo L, Chapuis Y. Endoscopic ultrasonography for the preoperative localization of insulinomas. Pancreas. 1996;13:55–60. - PubMed
LinkOut - more resources
Full Text Sources