

doi: 10.1102/1470-7330.2004.0018.
Magnetic Resonance Imaging of cholangiocarcinoma
Affiliations
- PMID: 18250017
- PMCID: PMC1434592
- DOI: 10.1102/1470-7330.2004.0018
Item in Clipboard
Magnetic Resonance Imaging of cholangiocarcinoma
Cancer Imaging.
.
Abstract
Preoperative imaging with MRI/MRA/MRCP is an accurate non-invasive method for staging cholangiocarcinoma,and determining resectability. It provides information regarding tumor size, extent of bile duct involvement, vascular patency, extrahepatic extension, nodal or distant metastases, and the presence of lobar atrophy. MRCP is better for demonstrating bile ducts distal to the stricture, although with ERCP, therapeutic intervention such as stent placement and biopsy can be performed.
Figures

Intrahepatic cholangiocarcinoma in a 35-year-old female who presented with right upper quadrant abdominal pain and no prior medical history. There is a large lobulated mass (arrow) in the right lobe of the liver, which, compared to liver parenchyma, is hypointense on the (a) axial T1-weighted (T1W) in-phase spoiled gradient-echo (SGRE) image, and mildly hyperintense on the (b) axial T2-weighted (T2W) fast spin echo (FSE) with fat saturation image. The mass shows heterogeneous rim enhancement on the (c) arterial-dominant phase gadolinium-enhanced axial T1W 3D SGRE image with fat saturation, and fills in heterogeneously on the (d) delayed (15 min) gadolinium-enhanced axial T1W SGRE image. A presumed metastatic nodule (white open arrow) is seen in the lateral segment of the left lobe on an (e) axial T2W FSE with fat suppression image. CT guided biopsy of the dominant mass revealed a cholangiocarcinoma.
Perihilar cholangiocarcinoma (Klatskin tumor) in a 62-year-old female presenting with painless jaundice. There is mass (arrow) at the junction of the main right and left hepatic ducts. The mass is seen on (a) an MRCP image as a focal stricture involving the duct bifurcation with dilatation of the intrahepatic ducts, left more than right, due to the presence of a right intrabiliary stent. In (b) T1W in-phase SGRE, the mass is hypointense relative to liver parenchyma, and mildly hyperintense on (c) T2W FSE with fat suppression. A susceptibility artifact from the right intrahepatic stent is demonstrated (asterisk). The mass enhances progressively (d–g) following gadolinium administration: in (d) the arterial-dominant phase, (e) portal-venous phase, (f) interstitial phase (2 min post-gadolinium), and is best depicted on (g) the 15 min post-gadolinium image as a hyperintense mass relative to adjacent liver parenchyma.

Intraductal cholangiocarcinoma in a 70-year-old male who presented with jaundice. An intraductal mass was found on ERCP. There is a minimally enhancing mass within the right main hepatic duct (arrow) on the (a) axial gadolinium-enhanced T1 SGRE image. The mass extends to the bifurcation of the ducts, and has resulted in intrahepatic ductal dilatation. The intraductal cholangiocarcinoma is seen as a filling defect (arrow) on the (b) coronal T2W SSFSE MRCP images. Cytology and brushings revealed a cholangiocarcinoma.
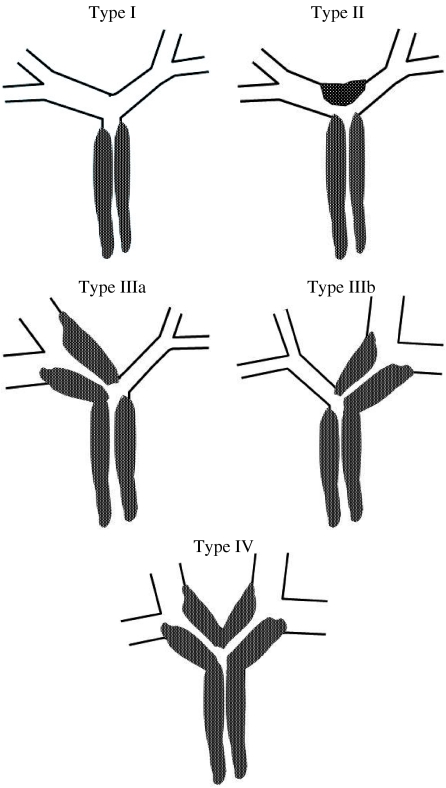
Schematic diagram of the Bismuth–Corlette classification scheme for perihilar tumors. Type I: tumor confined to CHD duct, obstructing the duct within 2 cm of the hilum. Type II: tumor of the CHD bifurcation involving both main right and left hepatic ducts, and causing obstruction at the hilum with no communication between the main right and left hepatic ducts. Type IIIa and IIIb: tumors extending into right and left secondary intrahepatic ducts, respectively, with absence of ductal obstruction on the contralateral side. Type IV: tumor involves the secondary and tertiary intrahepatic ducts in both lobes causing bilateral obstruction.

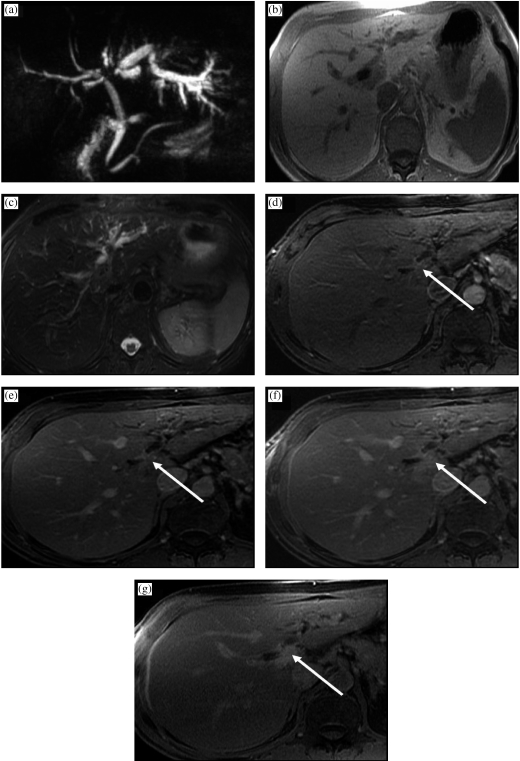
Inoperable perihilar cholangiocarcinoma in a 64-year-old female who presented with painless jaundice and had focal stenosis of the common bile duct on ERCP. There is a perihilar mass (arrow), which is hypointense to liver on (a) axial T1W in-phase SGRE, mildly hyperintense on (b) T2W FSE with fat saturation, has little to no arterial enhancement on (c) the arterial-dominant phase gadolinium-enhanced axial T1W 3D SGRE, mild enhancement on the (d) 2 min post-gadolinium image, and the tumor becomes mildly hyperintense to liver on the (e) 15 min post-gadolinium image. The tumor surrounds and narrows the main portal vein (white open arrow), and the right main hepatic artery (black open arrow) on a (f) higher slice. (g) Coronal thick slab T2W single shot fast spin-echo (SSFSE) MRCP image demonstrates long segment narrowing of the common hepatic and proximal common bile duct, with a stent traversing the stenotic segment as well as dilation of the intrahepatic bile ducts. (h) A corresponding minimum intensity projection (Min IP) reformatted image demonstrates the mildly enhancing mass surrounding the narrowed segment of common hepatic duct (curved arrow).
Similar articles
-
Differentiation of extrahepatic bile duct cholangiocarcinoma from benign stricture: findings at MRCP versus ERCP.Radiology. 2004 Oct;233(1):234-40. doi: 10.1148/radiol.2331031446. Epub 2004 Aug 27. Radiology. 2004. PMID: 15333766
-
Selective MRCP and CT-targeted drainage of malignant hilar biliary obstruction with self-expanding metallic stents.Gastrointest Endosc. 2003 Jul;58(1):41-9. doi: 10.1067/mge.2003.292. Gastrointest Endosc. 2003. PMID: 12838219
-
Malignant obstructive jaundice: comparison of MRCP and ERCP in the evaluation of distal lesions.Radiol Med. 2003 May-Jun;105(5-6):445-53. Radiol Med. 2003. PMID: 12949455 English, Italian.
-
Hilar cholangiocarcinoma: MRI/MRCP in staging and treatment planning.Abdom Imaging. 2008 Jul-Aug;33(4):444-51. doi: 10.1007/s00261-007-9281-6. Abdom Imaging. 2008. PMID: 17638040 Review.
-
Staging of extrahepatic cholangiocarcinoma.Eur Radiol. 2008 Oct;18(10):2182-95. doi: 10.1007/s00330-008-1006-x. Epub 2008 May 6. Eur Radiol. 2008. PMID: 18458911 Review.
Cited by
-
A Cholangioblastic Variant of Cholangiocarcinoma.ACG Case Rep J. 2022 Feb 15;9(2):e00746. doi: 10.14309/crj.0000000000000746. eCollection 2022 Feb. ACG Case Rep J. 2022. PMID: 35187186 Free PMC article.
-
Gadoxetic acid magnetic-enhanced resonance imaging in the diagnosis of cholangiocarcinoma.World J Gastroenterol. 2020 Aug 7;26(29):4261-4271. doi: 10.3748/wjg.v26.i29.4261. World J Gastroenterol. 2020. PMID: 32848332 Free PMC article. Review.
-
Comparative diagnostic performance of [68 Ga]Ga-FAPI PET/CT and [18 F]FDGPET/CT in biliary tract cancers: a systematic review and meta-analysis.Eur J Nucl Med Mol Imaging. 2025 Sep;52(11):4200-4212. doi: 10.1007/s00259-025-07264-5. Epub 2025 Apr 11. Eur J Nucl Med Mol Imaging. 2025. PMID: 40214739 Review.
-
The diagnostic MRCP examination: overcoming technical challenges to ensure clinical success.Biomed Imaging Interv J. 2008 Oct;4(4):e28. doi: 10.2349/biij.4.4.e28. Epub 2008 Oct 1. Biomed Imaging Interv J. 2008. PMID: 21611015 Free PMC article.
-
Hepatobiliary Tumors: Update on Diagnosis and Management.J Clin Transl Hepatol. 2015 Sep 28;3(3):169-81. doi: 10.14218/JCTH.2015.00012. Epub 2015 Sep 15. J Clin Transl Hepatol. 2015. PMID: 26623263 Free PMC article. Review.
References
-
- Buetow P, Midkiff R. Primary malignant neoplasms in the adult. MRI Clin N Am. 1997;5(2):289–318. - PubMed
-
- Vilgrain V, Van Beers BE, Flejou JF, et al. Intrahepatic cholangiocarcinoma: MRI and pathologic correlation in 14 patients. J Comput Assist Tomogr. 1997;21(1):59–65. - PubMed
-
- Hamrick-Turner J, Abbitt PL, Ros PR. Intrahepatic cholangiocarcinoma: MR appearance. AJR Am J Roentgenol. 1992;158(1):77–9. - PubMed
-
- Szklaruk J, Tamm E, Charnsangavej C. Preoperative imaging of biliary tract cancers. Surg Oncol Clin N Am. 2002;11(4):865–76. - PubMed
-
- Craig JR, Peters RL, Edmonson HA. Atlas of Tumor Pathology. 2nd series, fascicle 26. Washington, DC: Armed Forces Institute of Pathology; 1988. Tumors of the liver and intrahepatic bile ducts; pp. 16B–43.
LinkOut - more resources
Full Text Sources