

Surgery for rotator cuff disease
- PMID: 18254085
- PMCID: PMC6464842
- DOI: 10.1002/14651858.CD005619.pub2
Surgery for rotator cuff disease
Update in
-
Subacromial decompression surgery for rotator cuff disease.Cochrane Database Syst Rev. 2019 Jan 17;1(1):CD005619. doi: 10.1002/14651858.CD005619.pub3. Cochrane Database Syst Rev. 2019. PMID: 30707445 Free PMC article.
Abstract
Background: This review is one in a series of Cochrane reviews of interventions for shoulder disorders.
Objectives: To determine the effectiveness and safety of surgery for rotator cuff disease.
Search strategy: We searched the Cochrane Controlled Trials Register, (The Cochrane Library Issue 1, 2006), MEDLINE, EMBASE, CINAHL, Sports Discus, Science Citation Index (Web of Science) in March 2006 unrestricted by date or language.
Selection criteria: Only studies described as randomised or quasi-randomised clinical trials (RCTs) studying participants with rotator cuff disease and surgical interventions compared to placebo, no treatment, or any other treatment were included.
Data collection and analysis: Two independent review authors assessed methodological quality of each included trial and extracted data.
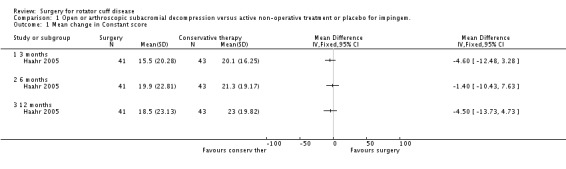
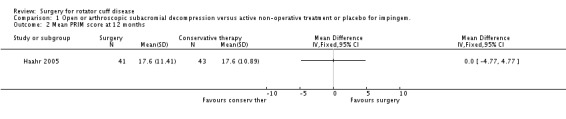
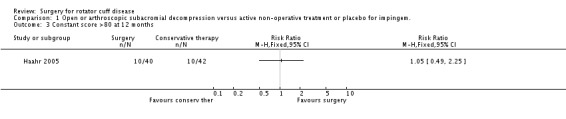
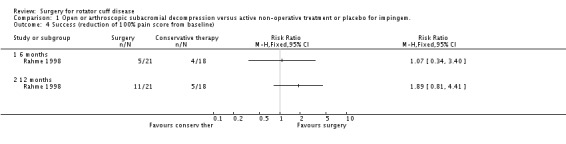
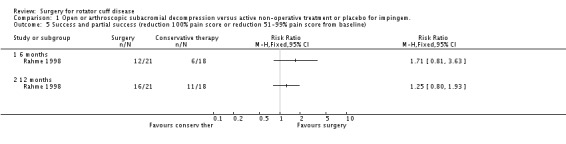
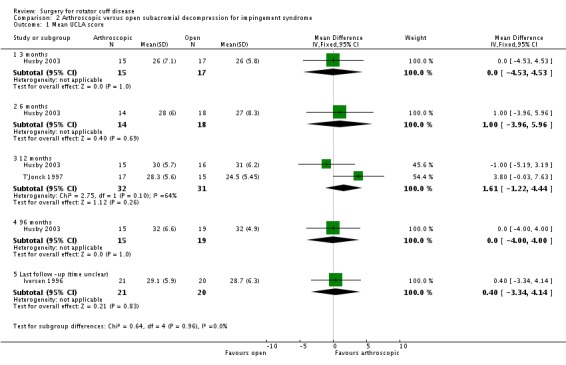
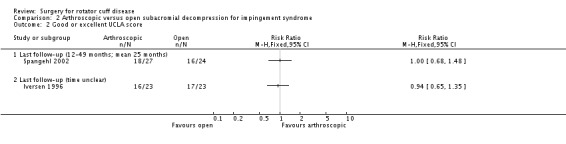
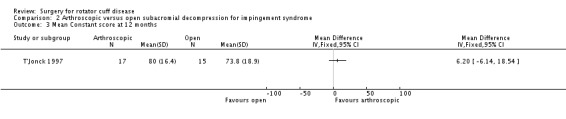
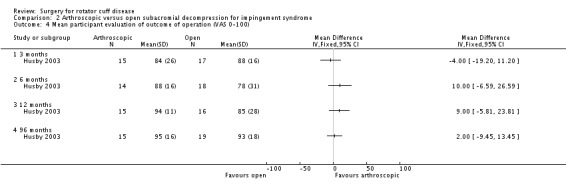
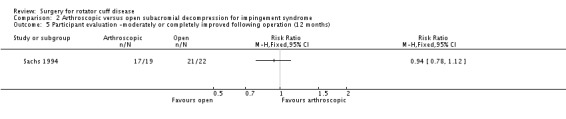
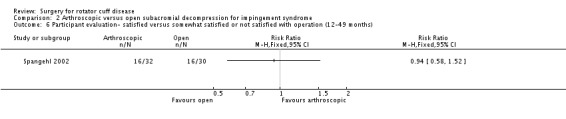
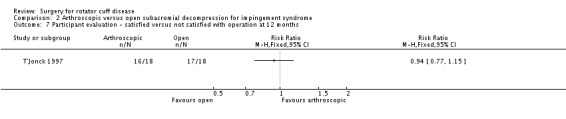
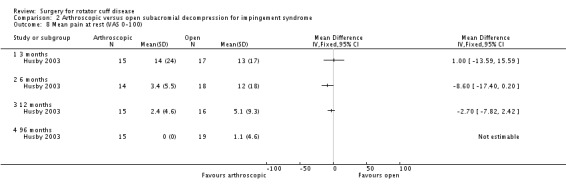
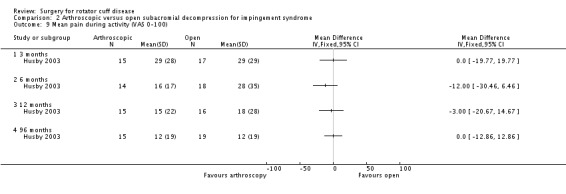
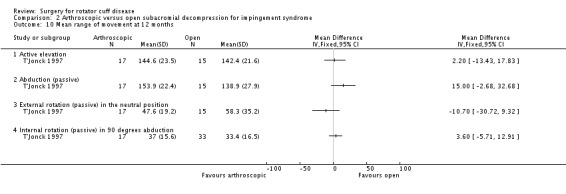
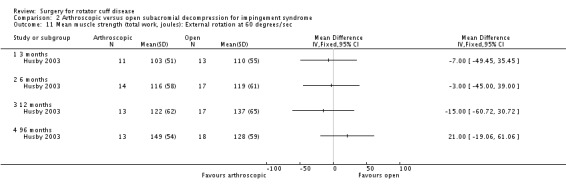
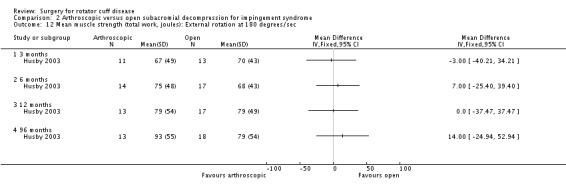
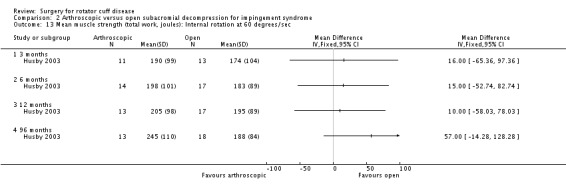
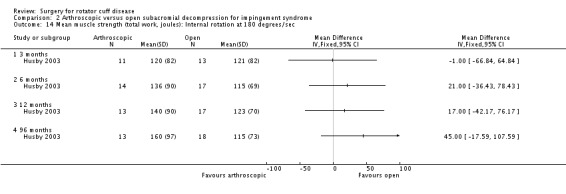
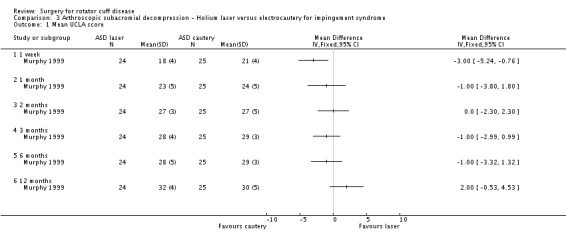
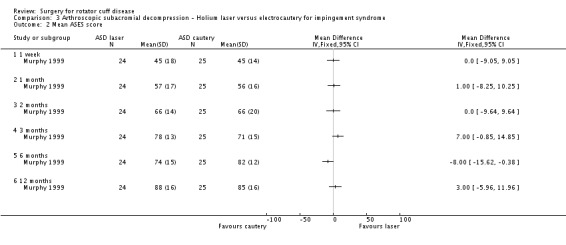
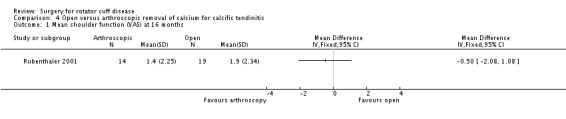
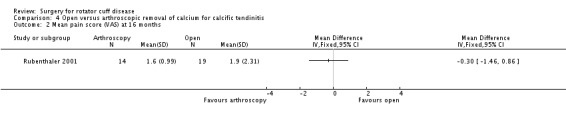
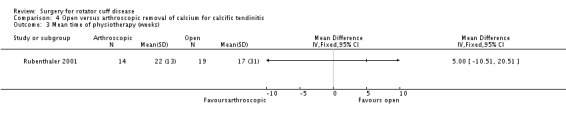
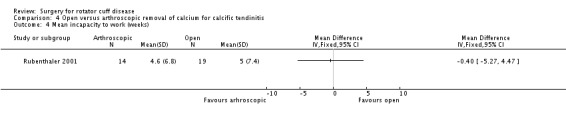
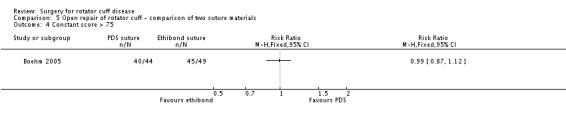
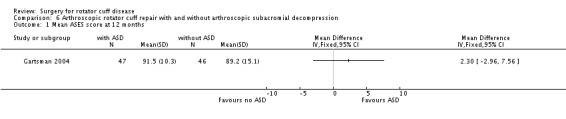
Main results: We included 14 RCTs involving 829 participants. Eleven trials included participants with impingement, two trials included participants with rotator cuff tear and one trial included participants with calcific tendinitis. No study met all methodological quality criteria and minimal pooling could be performed. Three trials compared either open or arthroscopic subacromial decompression with active non operative treatment (exercise programme, physiotherapy regimen of exercise and education, or graded physiotherapy strengthening program). No differences in outcome between these treatment groups were reported in any of these trials. One trial which also included a placebo arm (12 sessions detuned soft laser) reported that the Neer score of participants in both active treatment arms improved significantly more than those who received placebo at six months. Six trials that compared arthroscopic with open subacromial decompression reported no significant differences in outcome between groups at any time point although four trials reported a quicker recovery and/or return to work with arthroscopic decompression. Adverse events, which occurred in three trials and included infection, capsulitis, pain, deltoid atrophy, and reoperation, did not differ between surgical groups.
Authors' conclusions: Based upon our review of 14 trials examining heterogeneous interventions and all susceptible to bias, we cannot draw firm conclusions about the effectiveness or safety of surgery for rotator cuff disease. There is "Silver" (www.cochranemsk.org) level evidence from three trials that there are no significant differences in outcome between open or arthroscopic subacromial decompression and active non-operative treatment for impingement. There is also "Silver" level evidence from six trials that there are no significant differences in outcome between arthroscopic and open subacromial decompression although four trials reported earlier recovery with arthroscopic decompression.
Conflict of interest statement
No author in this review has any known conflict of interest in regard to this review. Simon Bell is an orthopaedic surgeon.
Figures
References
References to studies included in this review
-
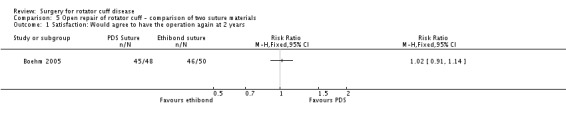
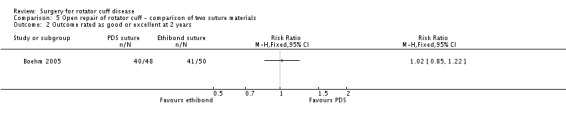
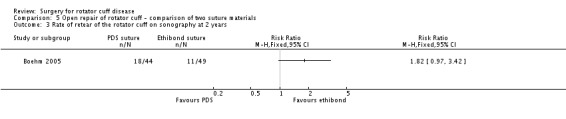
- Boehm TD, Werner A, Radtke S, Mueller T, Kirschner S, Gohlke F. The effect of suture materials and techniques on the outcome of repair of the rotator cuff. Journal of Bone and Joint Surgery (British) 2005;87‐B(6):819‐23. - PubMed
-
- Brox JI, Staff PH, Ljunggren AE, Brevik JI. Arthroscopic surgery compared with supervised exercises in patients with rotator cuff disease (stage 11 impingement syndrome). BMJ 1993;307:899‐903. - PMC - PubMed
- Brox JI, Uppheim G, Skagseth A, Brevik JI, Ljunggren AE, Staff PH. Arthroscopic surgery versus supervised exercises in patients with rotator cuff disease (stage 11 impingement syndrome): A prospective, randomized, controlled study in 125 patients with a 2 1/2 year follow‐uo. Journal of Shoulder and Elbow Surgery 1999;8(2):102‐11. - PubMed
-
- Gartsman GM, O'Connor DP. Arthroscopic rotator cuff repair with and without arthroscopic subacromial decompression: A prospective, randomized study of one‐year outcomes. Journal of shoulder and elbow surgery 2004;13(4):424‐6. - PubMed
-
- Haahr JP, Andersen JH. Exercises may be as efficient as subacromial decompression in patients with subacromial stage II impingement: 4–8‐years’ follow‐up in a prospective, randomized study. Scandinavian Journal of Rheumatology 2006;35:224‐8. - PubMed
- Haahr JP, Ostergaard S, Dalsgaard J, Norup K, Frost P, Lausen S, et al. Exercises versus arthroscopic decompression in patients with subacromial impingement: a randomised, controlled study in 90 cases with a one year follow up. Annals of the Rheumatic Diseases 2005;64(5):760‐4. - PMC - PubMed
-
- Husby T, Haugstvedt J‐R, Brandt M, Holm I, Steen H. Open versus arthroscopic subacromial decompression : A prospective, randomized study of 34 patients followed for 8 years. Acta Orthopaedica Scandinavica 2003;74(4):408‐14. - PubMed
References to studies excluded from this review
-
- Alvarez M, Litchfield R, Jackowski D, Griffin S, Kirkley A. A prospective, double blind randomized clinical trial comparing subacromial injection of betamethasone and xylocaine to xylocaine alone in chronic rotator cuff tendinosis. The American Journal of Sports Medicine 2005;33(2):255‐62. - PubMed
-
- Anderson, NH, Sojberg JO, Johannsen HV, Sneppen O. Self‐ training versus physiotherapist‐ supervised rehabilitation of the shoulder in patients treated with arthroscopic subacromial decompression: A clinical randomized study. Journal of Shoulder and Elbow Surgery 1999;8(2):99‐101. - PubMed
-
- Boileau P, Avidor C, Krishnan SG, Walch G, Kempf J‐F, Mole D. Cemented polyethylene versus uncemented metal‐ backed glenoid components in a total shoulder arthrosplasty: A prospective, double‐blind, randomized study. Journal of Shoulder and Elbow Surgery 2002;11(4):351‐9. - PubMed
-
- Bottoni CR, Wilckens JH, DeBerardino TM, D'Alleyrand J‐C, Rooney RC, Harpstrite JK, et al. A Prospective, Randomized Evaluation of Arthroscopic Stabilization versus Nonoperative Treatment in Patients with Acute, Traumatic, First‐ Tme Shoulder Disloations. The American Journal of Sports Medicine 2002;30(4):576‐80. - PubMed
-
- Connor PM, Yamaguchi K, Pollack RG, Flatlow EL, Bigliani LU. Comparison of arthoscopic and open revision decompression for failed anterior acromioplasty. Orthopedics 23;6:549‐54. - PubMed
References to studies awaiting assessment
-
- Jian X, Guodqing C, Jianquan W. Arthroscopically assisted mini‐open rotator cuff repair. The 5th Academic Congress of the Asian Shoulder Association 2005 Beijing (Conference proceedings). ACASA 2005 Beijing, September 2005:29.
-
- Xhao L, Xue Q, Zhang Y. Mini‐open vs. arthroscopic repair of full thickness tears of the supraspinatus: which one is better. The 5th Academic Congress of the Asian Shoulder Association 2005 Beijing ( Conference Proceedings). ACASA 2005 Beijing, September 2005:25.
Additional references
-
- Bjelle A. Epidemiology of shoulder problems. Baillieres Clinical Rheumatology 1989;3:437‐51. - PubMed
-
- Bridges‐Webb C, Britt H, Miles D, Neary S, Charles J, Traynor V. Morbidity and treatment in general practice in Australia 1990‐1991. Medical Journal of Australia 1992;Supplement 157:S1‐S56. - PubMed
-
- Chard MD, Hazelman R, Hazelman BL, King RH, Reiss BB. Shoulder disorders in the elderly: a community survey. Arthritis and Rheumatism 1991;34(6):766‐9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous