

Continuous infusion versus intermittent bolus doses of indomethacin for patent ductus arteriosus closure in symptomatic preterm infants
- PMID: 18254092
- PMCID: PMC8912238
- DOI: 10.1002/14651858.CD006071.pub2
Continuous infusion versus intermittent bolus doses of indomethacin for patent ductus arteriosus closure in symptomatic preterm infants
Abstract
Background: Indomethacin is a prostaglandin inhibitor used for the prevention and the treatment of patent ductus arteriosus (PDA). Although a 3-dose schedule has been commonly used, there is no consensus on optimal dosage and duration of indomethacin therapy for PDA closure. There are potential adverse effects of indomethacin use in premature infants such as a reduction in cerebral, mesenteric and renal blood flow and platelet dysfunction. Administering indomethacin continuously over 36-hours has been suggested as a safer and more effective option to prevent such adverse effects.
Objectives: To compare the efficacy and safety of continuous infusion versus bolus administration of indomethacin in closing a symptomatic PDA in preterm infants.
Search strategy: The standard search strategy of Cochrane Neonatal Review was used: MEDLINE and EMBASE (1966 - March 2007), Cochrane Central Register of Controlled Trials (CENTRAL, The Cochrane Library, Issue 1, 2007), bibliographies of reviews and trials were examined for references to other trials, previous symposia proceedings published in Pediatric Research (Pediatric Academic Societies Annual Meeting Abstract Book, 1972 - 2006). No language restrictions were applied.
Selection criteria: Randomized and quasi-randomized controlled trials comparing continuous indomethacin infusion to bolus doses for closure of a symptomatic PDA in preterm infants with a symptomatic PDA diagnosed clinically and/or by echocardiography.
Data collection and analysis: The methodological quality of each study was assessed. Authors were contacted regarding missing data as well as to inquire about the outcomes that were not reported. Meta-analysis was performed to calculate relative risk (RR), risk difference (RD) and 95% confidence intervals (CI).
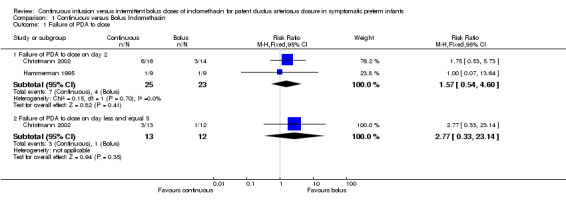
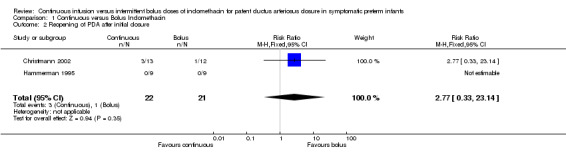
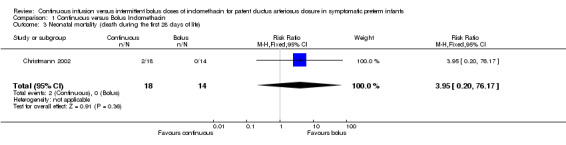
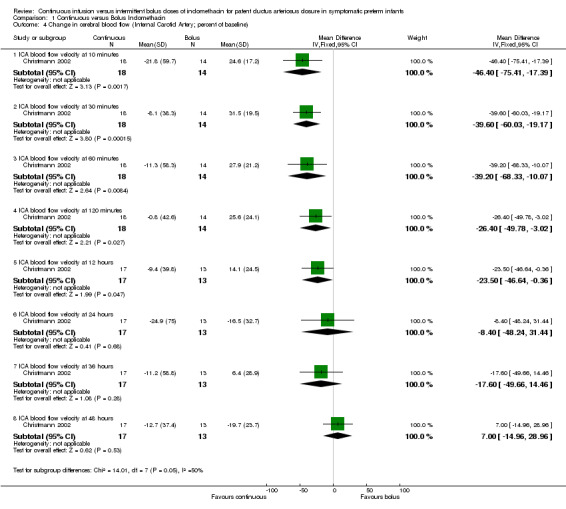
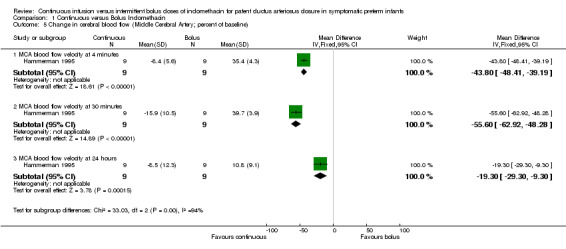
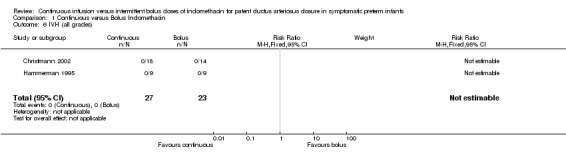
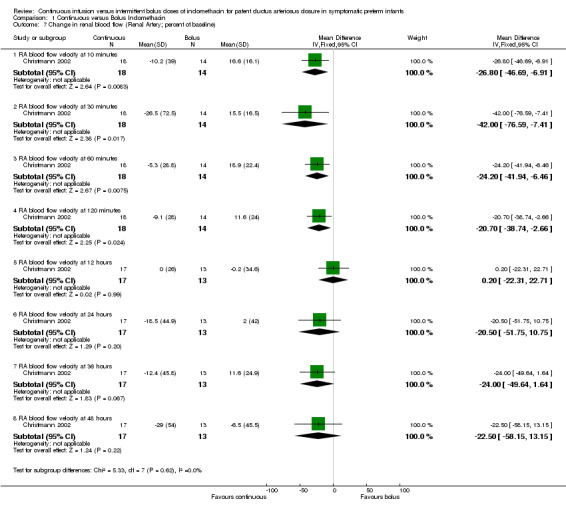
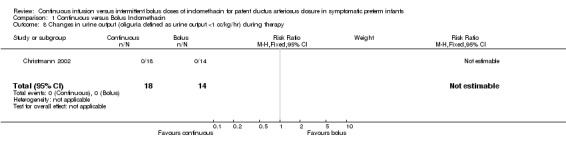
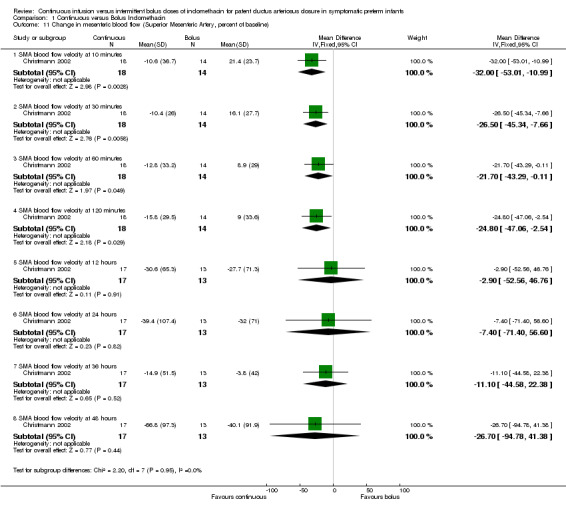
Main results: Only two small trials comparing continuous versus bolus indomethacin were eligible. Analysis of these studies showed that, although the primary outcome of PDA closure on days two and five slightly favored bolus administration, there was no statistical difference between the two groups. The estimates for PDA closure were RR 1.57 (95% CI 0.54, 4.60), RD 0.10 (95% CI -0.13, 0.33) for day 2 and RR 2.77 (95% CI 0.33, 23.14), RD 0.15 (95% CI -0.13, 0.42) for day five. There was no statistical difference between the bolus and continuous groups for the secondary outcomes of reopening of PDA, neonatal mortality, intraventricular hemorrhage (IVH) and necrotizing enterocolitis (NEC). These analyses were based on a very small number of events reported by these trials. None of the trials reported on outcomes such as requirement for retreatment with indomethacin or surgical ligation, mortality, bronchopulmonary dysplasia (BPD), retinopathy of prematurity (ROP), neurodevelopmental outcome and isolated intestinal perforation. The review demonstrated that there was a decrease in cerebral blood flow velocity after bolus injections and that the difference between the bolus and continuous infusion groups remained significant for 12 - 24 hour. In one study (Christmann 2002), the decrease in blood flow was maximum at 10 minutes [MD -46.40 (95% CI -75.41, -17.39)], while the other study (Hammerman 1995) reported a maximum drop at 30 minutes [MD -55.60 (95% CI -62.92, -48.28)]. Similar decrease in blood flow to the renal and mesenteric circulations following bolus administration was reported in one study (Christmann 2002). In both of these circulations, the decrease was maximum 30 minutes after the bolus injection [typical estimates for renal and mesenteric circulations, respectively: MD -42.00 (95% CI -76.59, -7.41) and MD -26.50 (95% CI -45.34, -7.66)] and lasted about two hours. None of the trials detected predefined levels of decreased urine output and increased levels of BUN and creatinine.
Authors' conclusions: Due to a paucity of events and lack of precision, the available data was found to be insufficient to draw conclusions regarding the efficacy of continuous indomethacin infusion versus bolus injections for the treatment of PDA. Although continuous indomethacin seems to cause less alterations in cerebral, renal and mesenteric circulations, the clinical meaning of this effect is unclear. Definitive recommendations about the preferred method of indomethacin administration i.e. continuous versus bolus infusions for the treatment of PDA in premature infants cannot be made based on the current findings of this review.
Conflict of interest statement
None
Figures
Update of
References
References to studies included in this review
Christmann 2002 {published data only}
-
- Christmann V, Liem KD, Semmekrot BA, Bor M. Changes in cerebral, renal and mesenteric blood flow velocity during continuous and bolus infusion of indomethacin. Acta Paediatrica 2002;91:440‐6. - PubMed
Hammerman 1995 {published data only}
-
- Hammerman C, Glaser J, Schimmel MS, Ferber B, Kaplan M, Eidelman AI. Continuous versus multiple rapid infusions of indomethacin: effects on cerebral blood flow velocity. Pediatrics 1995;95:244‐8. - PubMed
Additional references
Austin 1992
Brook 1995
-
- Brook M, Heymann M. Patent ductus arteriosus. Heart Disease in Infants, Children and Adolescents including the Fetus and Young Adult. Williams and Wilkins, 1995.
Clyman 1996
-
- Clyman RI. Recommendation for the postnatal use of indomethacin: an analysis of four separate treatment strategies. Journal of Pediatrics 1996;128:601‐7. - PubMed
Colditz 1989
Cotton 1978
-
- Cotton RB, Stahlman MT, Bender HW, Graham TP, Catterton WZ, Kovar I. Randomized trial of early closure of symptomatic patent ductus arteriosus in small preterm infants. Journal of Pediatrics 1978;93:647‐51. - PubMed
de Vries 2005
-
- Vries KS, Jagroep FK, Jaarsma AS, Elzenga NJ, Bos AF. Continuous indomethacin infusion may be less effective than bolus infusion for ductal closure in very low birth weight infants. American Journal of Perinatology 2005;22:71‐5. - PubMed
Edwards 1990
-
- Edwards AD, Wyatt JS, Richardson C, Potter A, Cope M, Delpy DT, Reynolds EO. Effects of indomethacin on cerebral haemodynamics in very preterm infants. Lancet 1990;335:1491‐5. - PubMed
Evans 1987
-
- Evans DH, Levene MI, Archer LN. The effect of indomethacin on cerebral blood‐flow velocity in premature infants. Developmental Medicine and Child Neurology 1987;29:776‐82. - PubMed
Fowlie 2002
Friedman 1976
-
- Friedman WF, Hirschklau MJ, Printz MP, Pitlick PT, Kirkpatrick SE. Pharmacologic closure of patent ductus arteriosus in the premature infant. New England Journal of Mediciine 1976;295:526‐9. - PubMed
Gersony 1983
-
- Gersony WM, Peckham GJ, Ellison RC, Miettinen OS, Nadas AS. Effects of indomethacin in premature infants with patent ductus arteriosus: results of a national collaborative study. Journal of Pediatrics 1983;102:895‐906. - PubMed
Herrera 2001
Lago 2002
-
- Lago P, Bettiol T, Salvadori S, Pitassi I, Vianello A, Chiandetti L, Saia OS. Safety and efficacy of ibuprofen versus indomethacin in preterm infants treated for patent ductus arteriosus: a randomised controlled trial. European Journal of Pediatrics 2002;161:202‐7. - PubMed
Laudignon 1988
-
- Laudignon N, Chemtob S, Bard H, Aranda JV. Effect of indomethacin on cerebral blood flow velocity of premature newborns. Biology of the Neonate 1988;54:254‐62. - PubMed
Mardoum 1991
-
- Mardoum R, Bejar R, Merritt AT, Berry C. Controlled study of the effects of indomethacin on cerebral blood flow velocities in newborn infants. Journal of Pediatrics 1991;118:112‐5. - PubMed
Ment 1988
-
- Ment LR, Duncan CC, Ehrenkranz RA, Kleinman CS, Taylor KJ, Scott DT, Gettner P, Sherwonit E, Williams J. Randomized low‐dose indomethacin trial for prevention of intraventricular hemorrhage in very low birth weight neonates. Journal of Pediatrics 1988;112:948‐55. - PubMed
Ment 1993
-
- Ment LR, Oh W, Ehrenkranz RA, Philip AG, Schneider K, Katz KH, Taylor KJ, Duncan CC, Makuch RW. Risk period for intraventricular hemorrhage of the preterm neonate is independent of gestational age. Seminars in Perinatology 1993;17:338‐41. - PubMed
Nehgme 1992
-
- Nehgme RA, O'Connor TZ, Lister G, Bracken MB. Patent ductus arteriosus. In: Sinclair JC, Bracken MB editor(s). Effective Care of the Newborn Infant. Oxford: Oxford University Press, 1992:281‐324.
Pezzati 1999
-
- Pezzati M, Vangi V, Biagiotti R, Bertini G, Cianciulli D, Rubaltelli FF. Effects of indomethacin and ibuprofen on mesenteric and renal blood flow in preterm infants with patent ductus arteriosus. Journal of Pediatrics 1999;135:733‐8. - PubMed
Shaffer 2002
-
- Shaffer CL, Gal P, Ransom JL, Carlos RQ, Smith MS, Davey AM, Dimaguila MA, Brown YL, Schall SA. Effect of age and birth weight on indomethacin pharmacodynamics in neonates treated for patent ductus arteriosus. Critical Care Medicine 2002;30:343‐8. - PubMed
Shah 2003
Siassi 1976
-
- Siassi B, Blanco C, Cabal LA, Coran AG. Incidence and clinical features of patent ductus arteriosus in low‐birthweight infants: a prospective analysis of 150 consecutively born infants. Pediatrics 1976;57:347‐51. - PubMed
Simko 1994
-
- Simko A, Mardoum R, Merritt TA, Bejar R. Effects on cerebral blood flow velocities of slow and rapid infusion of indomethacin. Journal of Perinatology 1994;14:29‐35. - PubMed
van Bel 1989
-
- Bel F, Bor M, Stijnen T, Baan J, Ruys JH. Cerebral blood flow velocity changes in preterm infants after a single dose of indomethacin: duration of its effect. Pediatrics 1989;84:802‐7. - PubMed
van Bel 1990
-
- Bel F, Zoeren D, Schipper J, Guit GL, Baan J. Effect of indomethacin on superior mesenteric artery blood flow velocity in preterm infants. Journal of Pediatrics 1990;116:965‐70. - PubMed
van Bel 1991
-
- Bel F, Guit GL, Schipper J, Bor M, Baan J. Indomethacin‐induced changes in renal blood flow velocity waveform in premature infants investigated with color Doppler imaging. Journal of Pediatrics 1991;118:621‐6. - PubMed
References to other published versions of this review
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous