

Lack of A1 adenosine receptors augments diabetic hyperfiltration and glomerular injury
- PMID: 18256360
- PMCID: PMC2390969
- DOI: 10.1681/ASN.2007060721
Lack of A1 adenosine receptors augments diabetic hyperfiltration and glomerular injury
Abstract
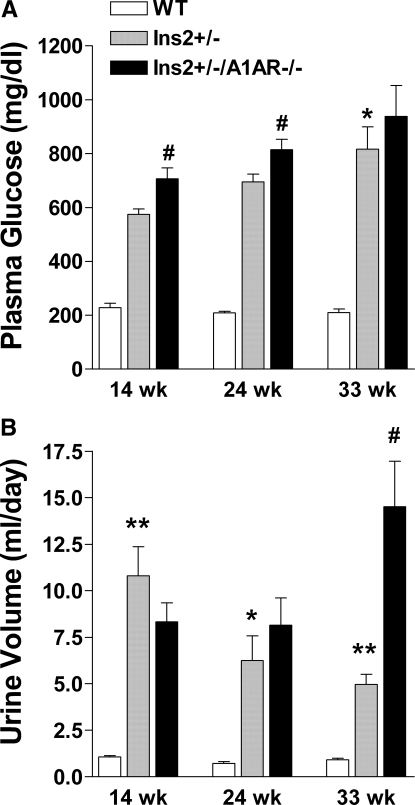
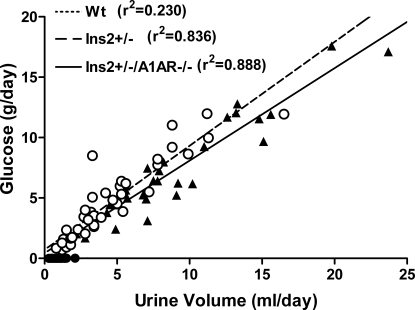
Intraglomerular hypertension and glomerular hyperfiltration likely contribute to the pathogenesis of diabetic nephropathy, and tubuloglomerular feedback (TGF) has been suggested to play a role in diabetic hyperfiltration. A1 adenosine receptor (A1AR) null mice lack a TGF response, so this model was used to investigate the contribution of TGF to hyperfiltration in diabetic Ins2(+/-) Akita mice. TGF responses in Ins2(+/-) A1AR(-/-) double mutants were abolished, whereas they were attenuated in Ins2(+/-) mice. GFR, assessed at 14, 24, and 33 wk, was approximately 30% higher in Ins2(+/-) than in wild-type (WT) mice and increased further in Ins2(+/-) A1AR(-/-) mutants (P < 0.01 versus both WT and Ins2(+/-) mice at all ages). Histologic evidence of glomerular injury and urinary albumin excretion were more pronounced in double-mutant than single-mutant or WT mice. In summary, the marked elevation of GFR in diabetic mice that lack a TGF response indicates that TGF is not required to cause hyperfiltration in the Akita model of diabetes. Rather, an A1AR-dependent mechanism, possibly TGF, limits the degree of diabetic hyperfiltration and nephropathy.
Figures










References
-
- Hostetter TH, Rennke HG, Brenner BM: The case for intrarenal hypertension in the initiation and progression of diabetic and other glomerulopathies. Am J Med 72: 375–380, 1982 - PubMed
-
- O'Bryan GT, Hostetter TH: The renal hemodynamic basis of diabetic nephropathy. Semin Nephrol 17: 93–100, 1997 - PubMed
-
- Woods LL, Mizelle HL, Hall JE: Control of renal hemodynamics in hyperglycemia: Possible role of tubuloglomerular feedback. Am J Physiol Renal Physiol 252: F65–F73, 1987 - PubMed
-
- Blantz RC, Konnen KS: Relation of distal tubular delivery and reabsorptive rate to nephron filtration. Am J Physiol Renal Physiol 233: F315–F24, 1977 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
