

Kidney transplantation as primary therapy for end-stage renal disease: a National Kidney Foundation/Kidney Disease Outcomes Quality Initiative (NKF/KDOQITM) conference
- PMID: 18256371
- PMCID: PMC2390948
- DOI: 10.2215/CJN.05021107
Kidney transplantation as primary therapy for end-stage renal disease: a National Kidney Foundation/Kidney Disease Outcomes Quality Initiative (NKF/KDOQITM) conference
Abstract
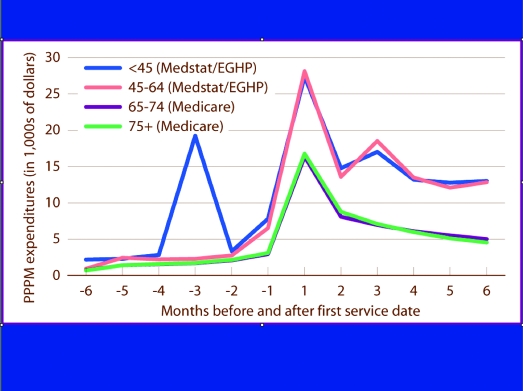
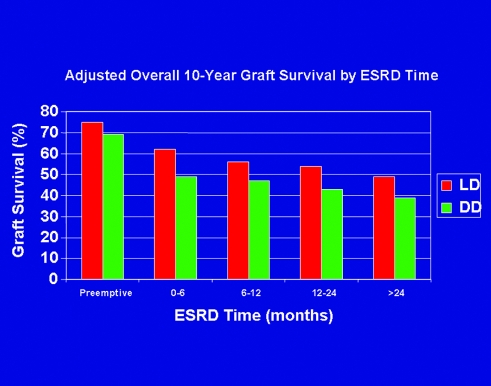
Background and objectives: Kidney transplantation is the most desired and cost-effective modality of renal replacement therapy for patients with irreversible chronic kidney failure (end-stage renal disease, stage 5 chronic kidney disease). Despite emerging evidence that the best outcomes accrue to patients who receive a transplant early in the course of renal replacement therapy, only 2.5% of incident patients with end-stage renal disease undergo transplantation as their initial modality of treatment, a figure largely unchanged for at least a decade.
Design, setting, participants, & measurements: The National Kidney Foundation convened a Kidney Disease Outcomes Quality Initiative (KDOQI) conference in Washington, DC, March 19 through 20, 2007, to examine the issue. Fifty-two participants representing transplant centers, dialysis providers, and payers were divided into three work groups to address the impact of early transplantation on the chronic kidney disease paradigm, educational needs of patients and professionals, and finances of renal replacement therapy.
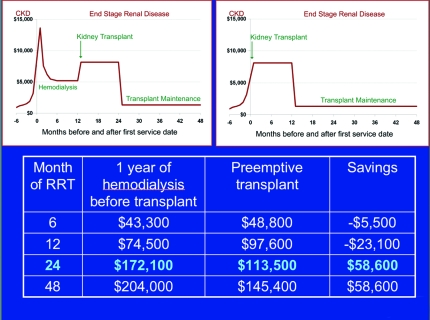
Results: Participants explored the benefits of early transplantation on costs and outcomes, identified current barriers (at multiple levels) that impede access to early transplantation, and recommended specific interventions to overcome those barriers.
Conclusions: With implementation of early education, referral to a transplant center coincident with creation of vascular access, timely transplant evaluation, and identification of potential living donors, early transplantation can be an option for substantially more patients with chronic kidney disease.
Figures
References
-
- Rennie D: Home dialysis and the costs of uremia. N Engl J Med 298: 399–400, 1978 - PubMed
-
- Wolfe RA, Ashby VB, Milford EL, Ojo AO, Ettenger RE, Agodoa LY, Held PJ, Port FK: Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. N Engl J Med 341: 1725–1730, 1999 - PubMed
-
- Ashby VB, Kalbfleisch JD, Wolfe RA, Lin MJ, Port FK, Leichtman AB: Geographic variability in access to primary kidney transplantation in the United States, 1996–2005. Am J Transplant 7[Suppl 1]: 1412–1423, 2007 - PubMed
-
- Meier-Kriesche HU, Port FK, Ojo AO, Rudich SM, Hanson JA, Cibrik DM, Leichtman AB, Kaplan B: Effect of waiting time on renal transplant outcome. Kidney Int 58: 1311–1317, 2000 - PubMed
-
- US Renal Data System: USRDS 2006 Annual Data Report. Available at: http://www.usrds.org/adr_2006.htm. Accessed June 19, 2007
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
