

Hemodialysis arteriovenous fistula patency revisited: results of a prospective, multicenter initiative
- PMID: 18256379
- PMCID: PMC2386712
- DOI: 10.2215/CJN.02950707
Hemodialysis arteriovenous fistula patency revisited: results of a prospective, multicenter initiative
Abstract
Background and objectives: Vascular access standards are predominantly based on older, single-center reports; however, the hemodialysis population has changed dramatically and primary arteriovenous fistula failure is a huge problem. This prospective, multicenter study used standardized definitions to analyze patency rates and potential risk factors that affect functional patency and late arteriovenous fistula functionality.
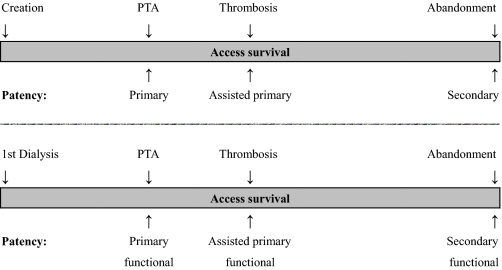
Design, setting, participants, & measurements: Eleven centers participated in a guidelines implementation program. All new permanent vascular accesses were included. Patency and functional patency, defined as access survival from creation and from first dialysis use, respectively, were calculated using Kaplan-Meier analysis. Risk factors for primary functional patency loss (intervention-free interval) and secondary failure (abandonment) were determined using regression models.
Results: A total of 491 arteriovenous fistulas were placed in 395 patients. Six-, 12-, and 18-mo secondary patency and functional patency were 75 +/- 2.0, 70 +/- 2.3, and 67 +/- 2.7% and 90 +/- 1.9, 88 +/- 2.2, and 86 +/- 2.7%, respectively. Primary failure rate was 40%. Thrombosis rate was 0.14 per patient-year. Diabetes and arteriovenous fistula surveillance were significantly associated with primary functional patency loss. Preoperative duplex was inversely related to secondary failure. The secondary failure rate per hospital varied from 0 to 39%.
Conclusions: This study showed a marked difference between patency and functional patency, likely to be explained by high primary failure rates. Hemodialysis patients with diabetes can be expected to have reduced primary functional patency rates, but if treated adequately, then arteriovenous fistula functionality can be maintained as long as in patients without diabetes.
Figures


References
-
- NKF-K/DOQI clinical practice guidelines for vascular access. Am J Kidney Dis 48[Suppl 1]: S248–S273, 2006 - PubMed
-
- NKF-K/DOQI clinical practice guidelines for vascular access. Am J Kidney Dis 48[Suppl 1]: S176–S247, 2006 - PubMed
-
- US Renal Data System: USRDS 2006 Annual Data Report: Atlas of End-Stage Renal Disease in the United States, Bethesda, National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, 2006
-
- Rostand SG, Gretes JC, Kirk KA, Rutsky EA, Andreoli TE: Ischemic heart disease in patients with uremia undergoing maintenance hemodialysis. Kidney Int 16: 600–611, 1979 - PubMed
-
- Pisoni RL, Young EW, Dykstra DM, Greenwood RN, Hecking E, Gillespie B, Wolfe RA, Goodkin DA, Held PJ: Vascular access use in Europe and the United States: Results from the DOPPS. Kidney Int 61: 305–316, 2002 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
