

What do we know about communicating risk? A brief review and suggestion for contextualising serious, but rare, risk, and the example of cox-2 selective and non-selective NSAIDs
- PMID: 18257914
- PMCID: PMC2374447
- DOI: 10.1186/ar2373
What do we know about communicating risk? A brief review and suggestion for contextualising serious, but rare, risk, and the example of cox-2 selective and non-selective NSAIDs
Abstract
Background: Communicating risk is difficult. Although different methods have been proposed - using numbers, words, pictures or combinations - none has been extensively tested. We used electronic and bibliographic searches to review evidence concerning risk perception and presentation. People tend to underestimate common risk and overestimate rare risk; they respond to risks primarily on the basis of emotion rather than facts, seem to be risk averse when faced with medical interventions, and want information on even the rarest of adverse events.
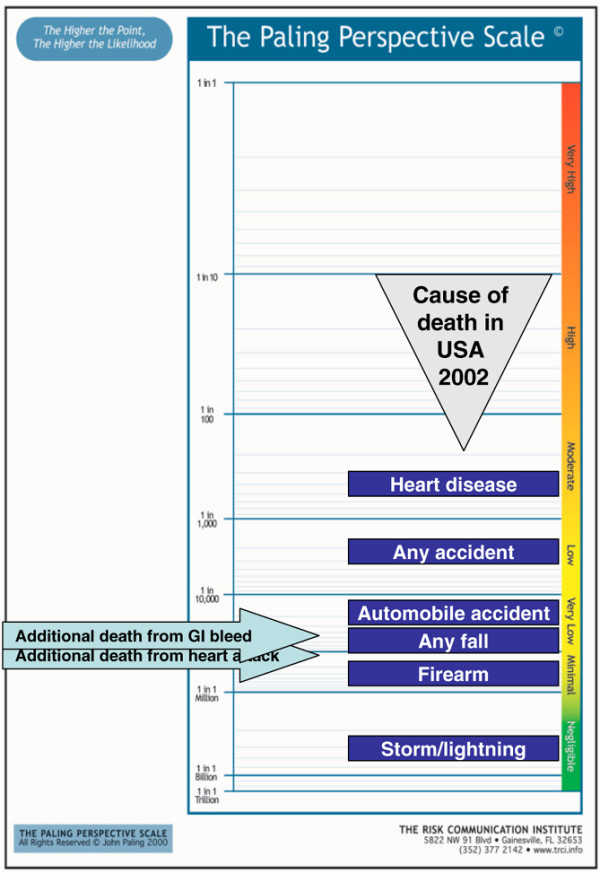
Methods: We identified observational studies (primarily in the form of meta-analyses) with information on individual non-steroidal anti-inflammatory drug (NSAID) or selective cyclooxygenase-2 inhibitor (coxib) use and relative risk of gastrointestinal bleed or cardiovascular event, the background rate of events in the absence of NSAID or coxib, and the likelihood of death from an event. Using this information we present the outcome of additional risk of death from gastrointestinal bleed and cardiovascular event for individual NSAIDs and coxibs alongside information about death from other causes in a series of perspective scales.
Results: The literature on communicating risk to patients is limited. There are problems with literacy, numeracy and the human tendency to overestimate rare risk and underestimate common risk. There is inconsistency in how people translate between numbers and words. We present a method of communicating information about serious risks using the common outcome of death, using pictures, numbers and words, and contextualising the information. The use of this method for gastrointestinal and cardiovascular harm with NSAIDs and coxibs shows differences between individual NSAIDs and coxibs.
Conclusion: Although contextualised risk information can be provided on two possible adverse events, many other possible adverse events with potential serious consequences were omitted. Patients and professionals want much information about risks of medical interventions but we do not know how best to meet expectations. The impact of contextualised information remains to be tested.
Figures












References
-
- Berry D. Risk, Communication, and Health Psychology. Maidenhead, UK: Open University Press; 2004.
-
- Kearney PM, Baigent C, Godwin J, Halls H, Emberson JR, Patrono C. Do selective cyclo-oxygenase-2 inhibitors and traditional non-steroidal anti-inflammatory drugs increase the risk of atherothrombosis? Meta-analysis of randomised trials. BMJ. 2006;332:1302–1308. doi: 10.1136/bmj.332.7553.1302. - DOI - PMC - PubMed
-
- Lewis SC, Langman MJ, Laporte JR, Matthews JN, Rawlins MD, Wiholm BE. Dose-response relationships between individual nonaspirinnonsteroidal anti-inflammatory drugs (NANSAIDs) and serious upper gastrointestinal bleeding: a meta-analysis based on individual patient data. Br J Clin Pharmacol. 2002;54:320–326. doi: 10.1046/j.1365-2125.2002.01636.x. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
