

Metabolic effects of enteral versus parenteral alanyl-glutamine dipeptide administration in critically ill patients receiving enteral feeding: a pilot study
- PMID: 18258342
- PMCID: PMC2692723
- DOI: 10.1016/j.clnu.2007.12.003
Metabolic effects of enteral versus parenteral alanyl-glutamine dipeptide administration in critically ill patients receiving enteral feeding: a pilot study
Abstract
Background: Glutamine (Gln) may become conditionally indispensable during critical illness. The short-term metabolic effects of enteral versus parenteral Gln supplementation are unknown in this clinical setting.
Objectives: We studied metabolic effects of intravenous (i.v.) alanyl-Gln dipeptide (AG) supplementation and enteral (e.n.) AG supplementation on plasma Gln concentration, antioxidant status, plasma lymphocyte subset number, gut permeability and nitrogen balance in adult critically ill patients requiring tube feeding compared to a control group not receiving Gln supplementation.
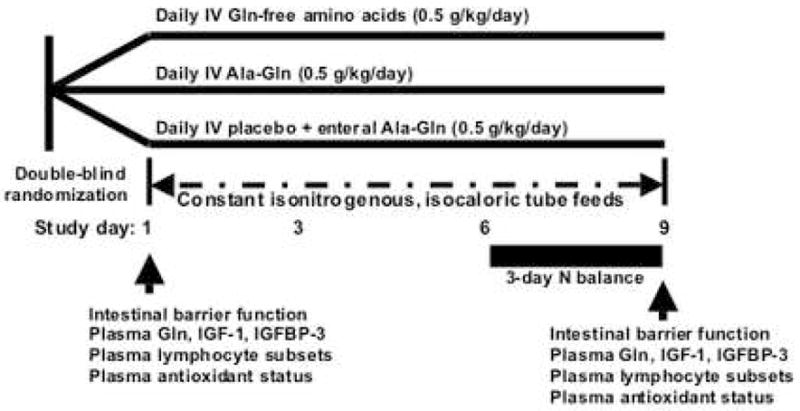
Methods: In a double-blind, pilot clinical trial, 44 medical and surgical ICU patients received identical Gln-free tube feedings 24 h/day and were randomized to either isonitrogenous control (n=15), e.n. AG (n=15) or i.v. AG (n=14) groups (AG). Twelve patients were discontinued from the study. The goal AG dose was 0.5 g/kg/day. Biochemical and metabolic endpoints were measured at baseline and on day 9 (plasma Gln, antioxidant indices, lymphocyte subsets; serum IGF-1 and IGF-binding protein-3; intestinal permeability). Nitrogen balance was determined between study days 6 and 8.
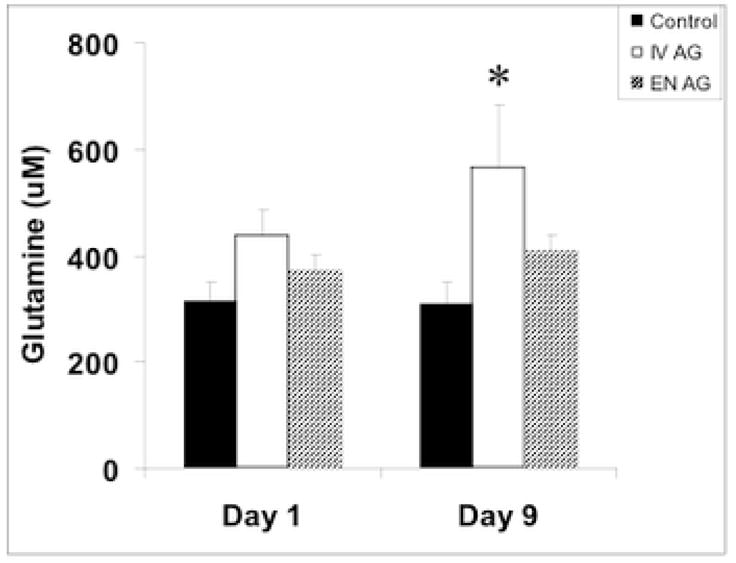
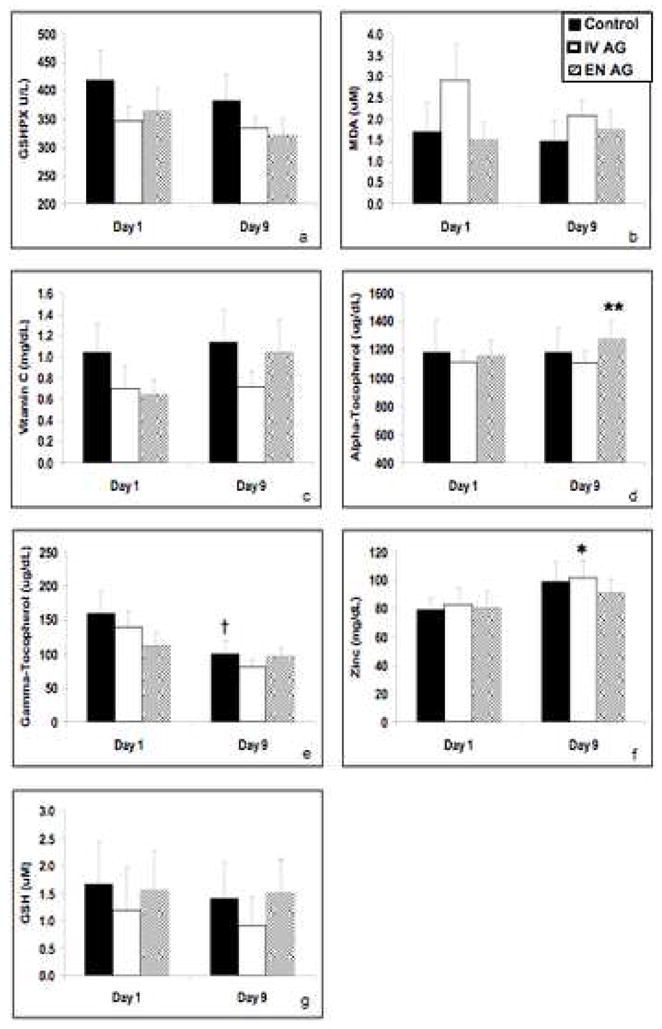
Results: Illness severity indices, clinical demographics, enteral energy and nitrogen intake and major biochemical indices were similar between groups during study. Plasma Gln was higher in the i.v. AG (565+/-119 microM, mean+/-SEM) vs the e.n. AG (411+/-27 microM) group by day 9 (p=0.039); however, subjects in the i.v. AG group received a higher dose of AG (i.v. AG 0.50 versus e.n. AG 0.32+/-0.02 g/kg/day; p<0.001). E.n. AG subjects showed a significant increase in plasma alpha-tocopherol levels over time and maintained plasma gamma-tocopherol concentrations. There were no differences between groups for plasma concentrations of vitamin C, glutathione, malondialdehyde (MDA), T-lymphocyte subsets, intestinal permeability or nitrogen balance.
Conclusions: This study showed that alanyl-Gln administration by enteral or parenteral routes did not appear to affect antioxidant capacity or oxidative stress markers, T-lymphocyte subset (CD-3, CD-4, CD-8) number, gut barrier function or whole-body protein metabolism compared to unsupplemented ICU patients requiring enteral tube feeding. Enteral Gln appeared to maintain plasma tocopherol levels in this pilot metabolic study.
Figures
References
-
- Debaveye Y, Van den Berghe G. Risks and benefits of nutritional support during critical illness. Annu Rev Nutr. 2006;26:513–538. - PubMed
-
- Crimi E, Sica V, Williams-Ignarro S, Zhang H, Slutsky AS, Ignarro LJ, et al. The role of oxidative stress in adult critical care. Free Radic Biol Med. 2006;40:398–406. - PubMed
-
- Bergstrom J, Furst P, Noree LO, Vinnars E. Intracellular free amino acid concentration in human muscle tissue. J Appl Physiol. 1974;36:693–697. - PubMed
-
- Boelens PG, Nijveldt RJ, Houdijk AP, Meijer S, van Leeuwen PA. Glutamine alimentation in catabolic states. J Nutr. 2001;131:2569S–2577S. - PubMed
-
- Wischmeyer PE. The glutamine story: where are we now? Curr Opin Crit Care. 2006;12:142–148. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
