

Endoscopic "no hole" full-thickness biopsy of the stomach to detect myenteric ganglia
- PMID: 18262183
- PMCID: PMC2814422
- DOI: 10.1016/j.gie.2007.10.017
Endoscopic "no hole" full-thickness biopsy of the stomach to detect myenteric ganglia
Abstract
Background: The etiology of several common gastric motility diseases remains largely unknown. Gastric wall biopsy specimens that include the muscularis propria to evaluate the enteric nervous system, interstitial cells of Cajal, and related cells are essential to promote our understanding of the pathophysiologic mechanisms. On the basis of our previous work, a double EMR technique provided sufficient tissue to identify myenteric ganglia. A serious limitation to the technique was the resultant gastric wall perforation after tissue resection. The optimal procedure would seal the gastric wall defect before tissue resection, eliminating the risk of peritonitis.
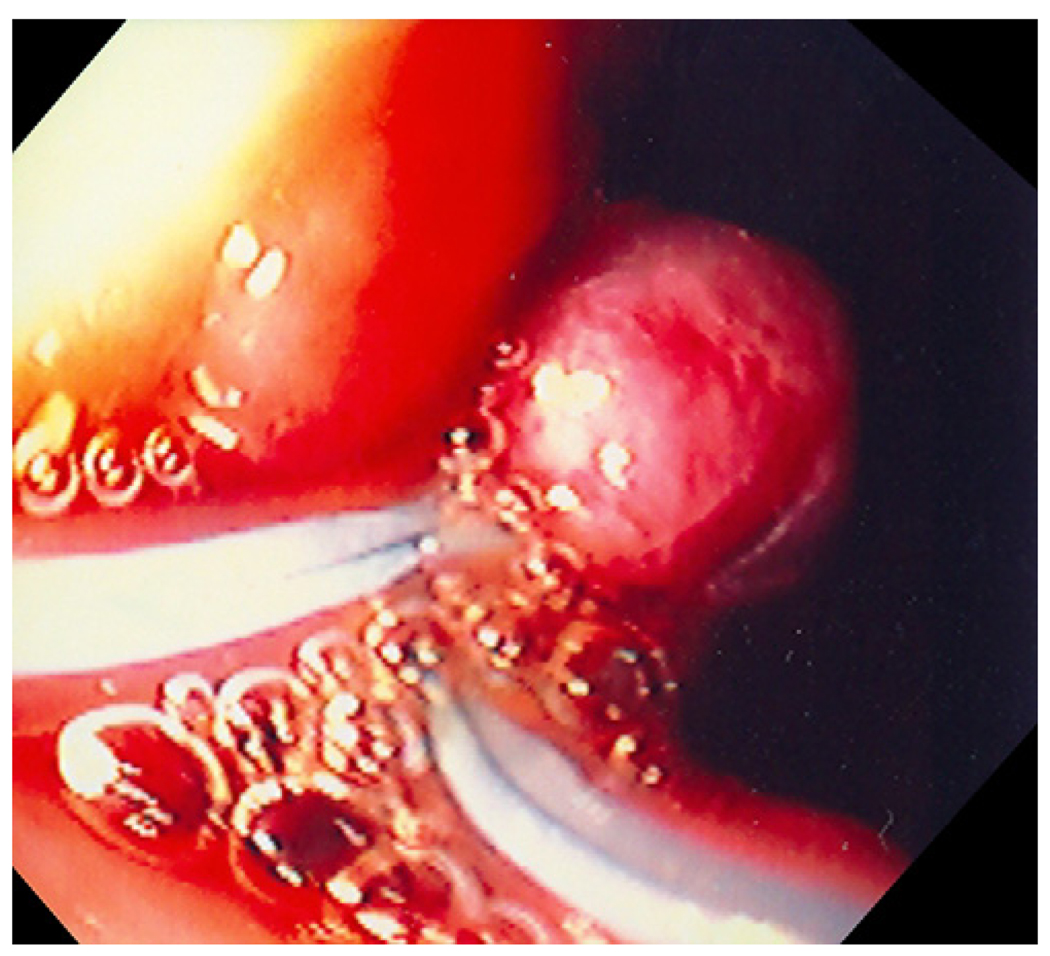
Objectives: The aims of this study were to (1) determine the technical feasibility and reproducibility of a full-thickness gastric biopsy by use of a novel double EMR technique without creating a perforation ("no hole") and to (2) determine safety of the procedure.
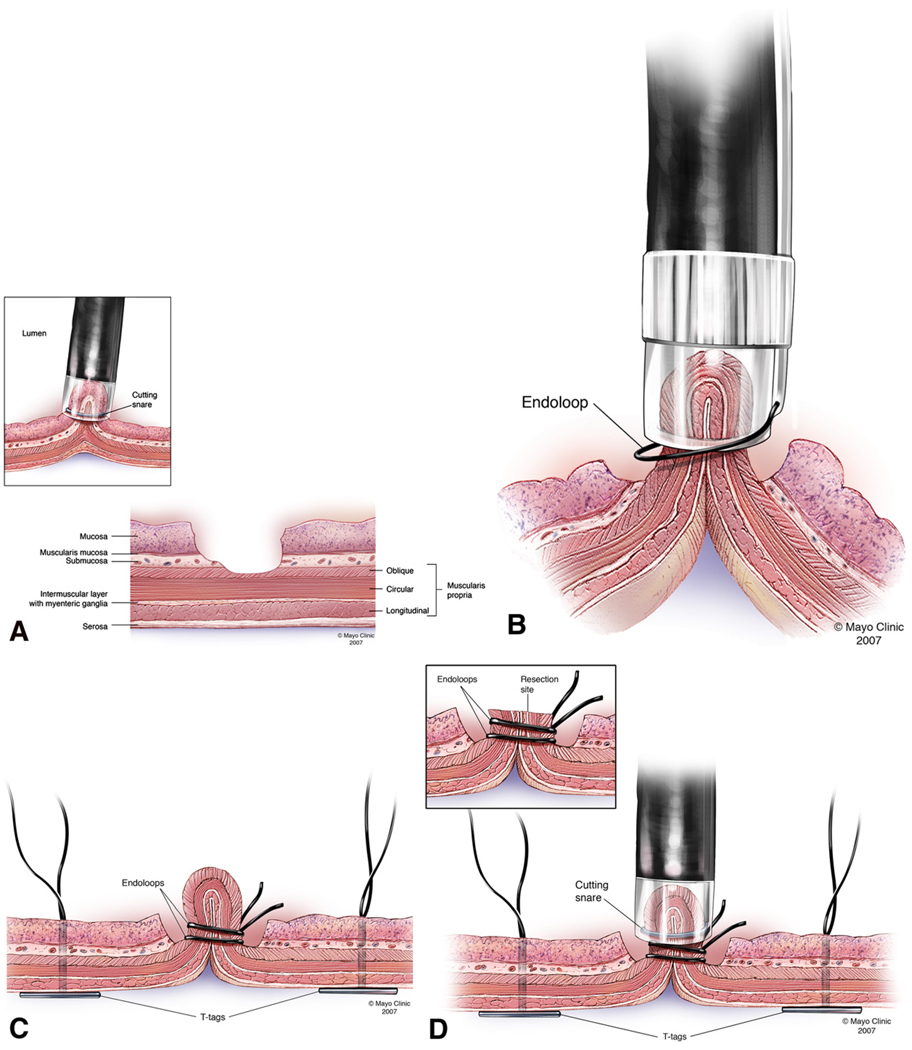
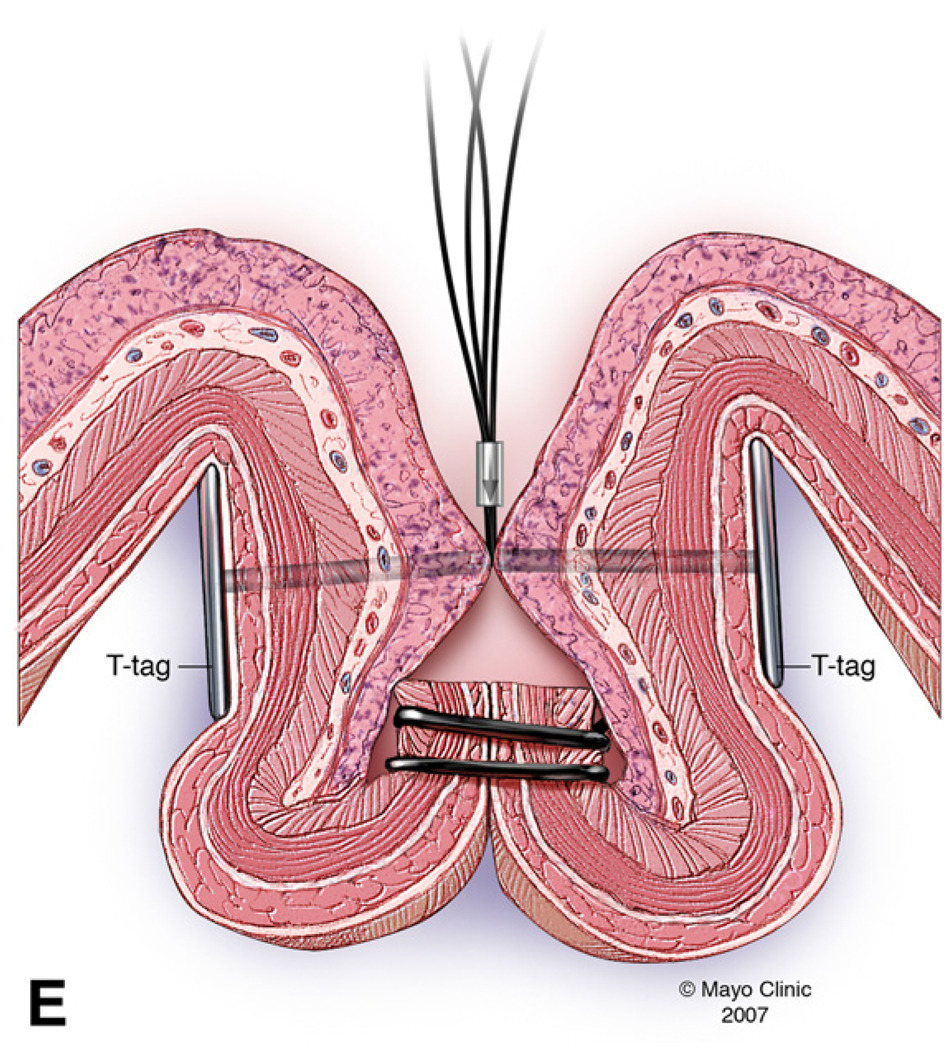
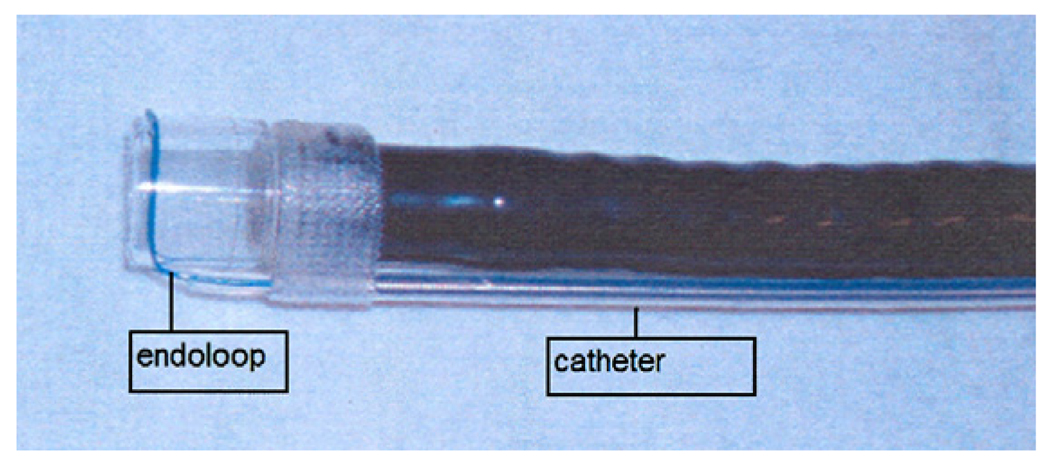
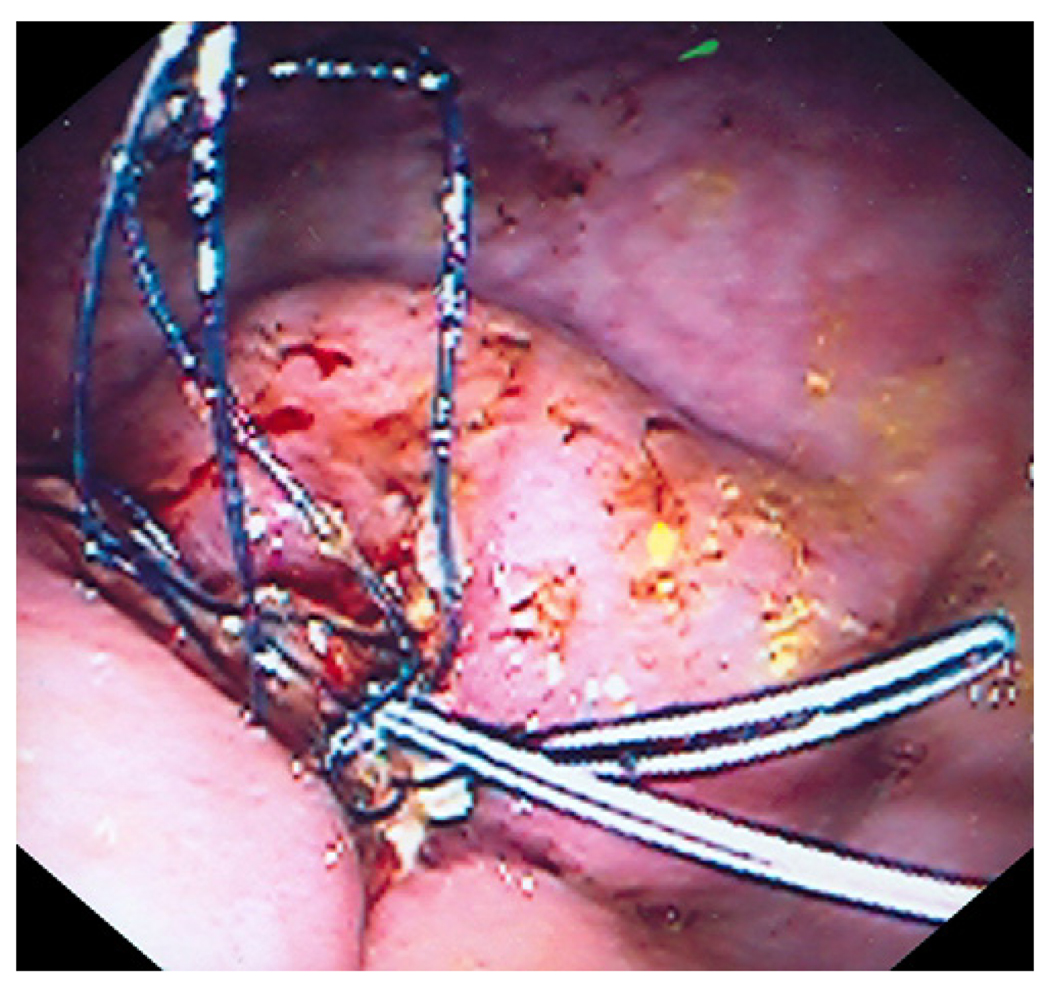
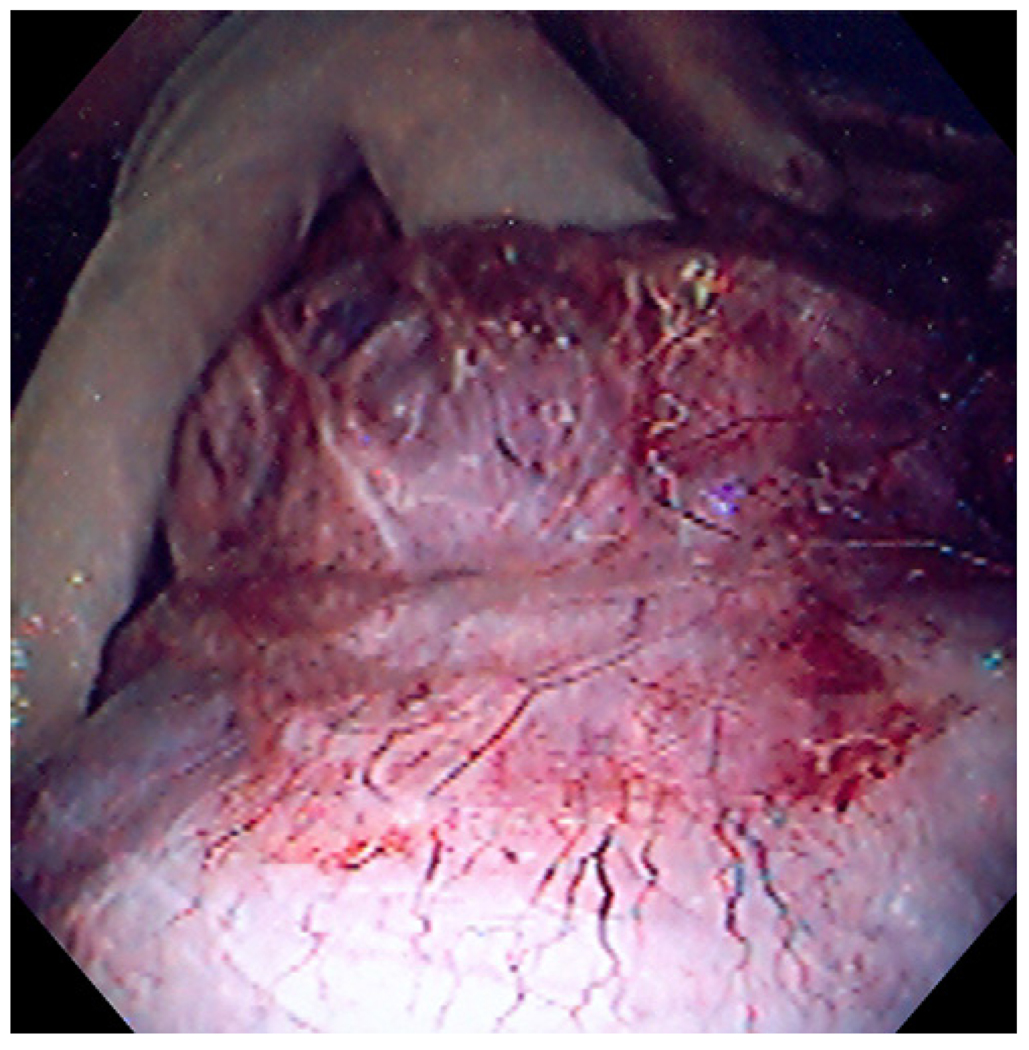
Design and interventions: Preclinical study of 6 pigs. Each animal underwent a "no hole" double EMR survival procedure. To prevent perforation, detachable endoloops and prototype T-tag tissue anchors were placed before resection. At 2 weeks repeat endoscopy was performed followed by necropsy.
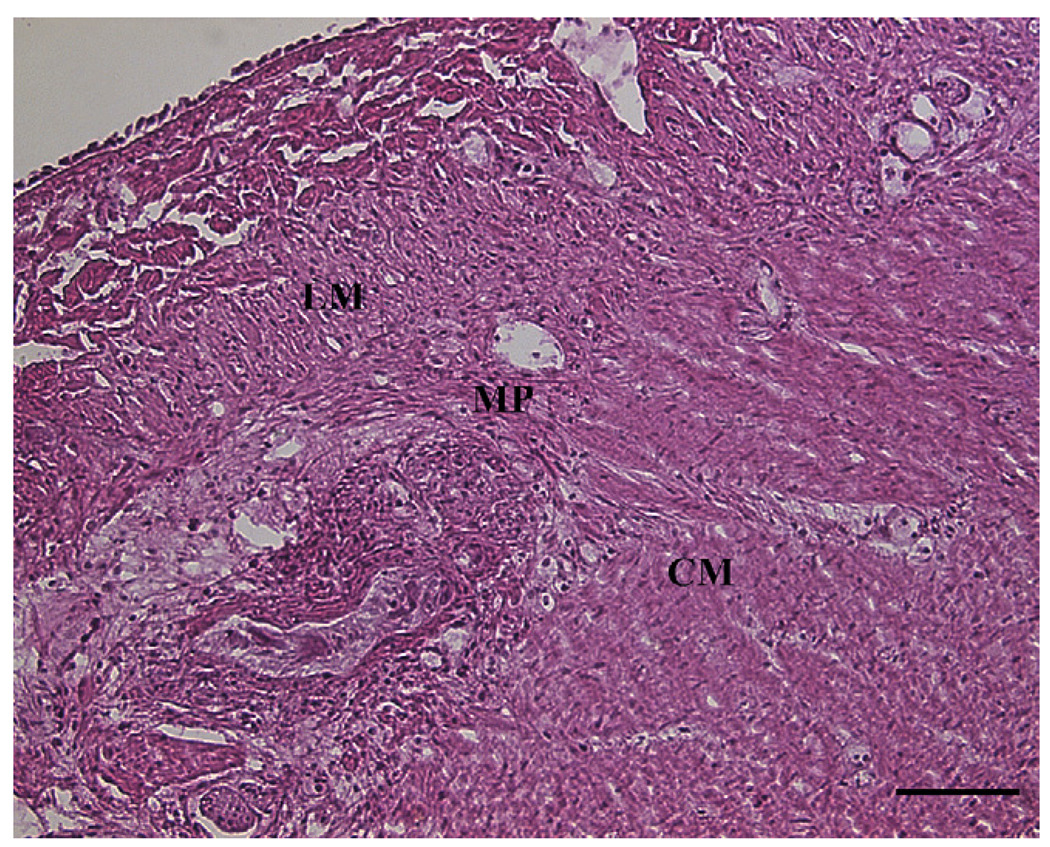
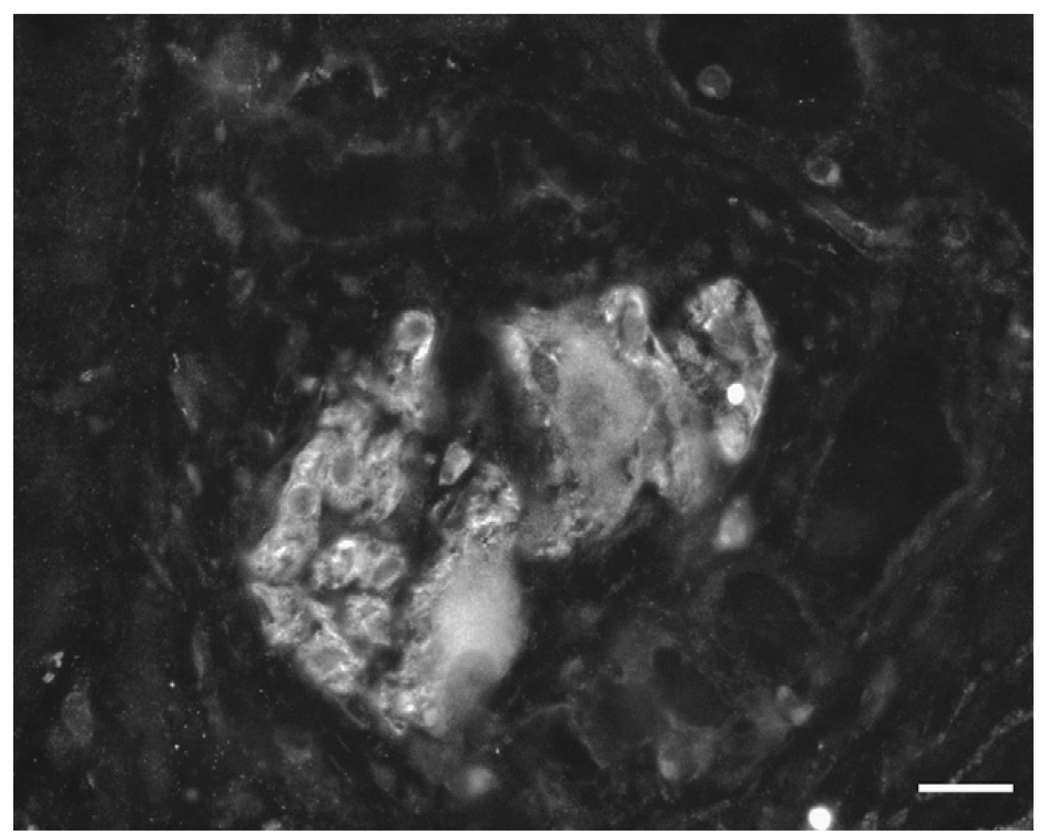
Main outcome measurements: Hematoxylin-eosin staining was used to determine which muscle layers were included in the resected specimen, and an antibody to neuronal nitric oxide synthase was used to visualize myenteric ganglia in the sample. Technical feasibility, reproducibility, and safety of the procedure were evaluated.
Results: Full-thickness gastric biopsy specimens were obtained from all animals without overt perforation. There were no procedural complications. Histologic examination showed muscularis propria with all layers of muscle present, and immunochemical studies demonstrated myenteric ganglia in all tissue samples. Four animals had an uneventful clinical course, and repeat endoscopy at week 2 showed ulceration with stellate fibrosis. Necropsy showed mild localized adhesions. Two animals were killed at days 3 and 6, respectively, because of suspected peritonitis. At necropsy, delayed perforations at the resection sites were noted with displaced endoloops and tissue anchors.
Conclusion: This study explored the concept of obtaining deep muscle wall biopsy specimens with use of a unique approach of resection without perforation. The novel "no hole" double EMR technique was technically feasible and reproducible with sufficient tissue obtained to identify myenteric ganglia. However, there was a high delayed perforation rate associated with displaced endoloops and tissue anchors. On the basis of this early experience, improved safety data may be anticipated with future studies using improved tissue closure devices.
Conflict of interest statement
Figures

Comment in
-
Full-thickness endoscopic sampling of the stomach wall as a technique to manage gastroparesis.Gastrointest Endosc. 2008 Aug;68(2):308-9. doi: 10.1016/j.gie.2008.02.069. Gastrointest Endosc. 2008. PMID: 18656598 No abstract available.
References
-
- Gershon MD, Tack J. The serotonin signaling system: from basic understanding to drug development for functional GI disorders. Gastroenterology. 2007;132(1):397–414. - PubMed
-
- Camilleri M. Clinical practice. Diabetic gastroparesis. N Engl J Med. 2007;356(8):820–829. - PubMed
-
- Rajan E, Gostout CJ, Lurken MS, Locke GR, Talley NJ, Szarka LA, et al. Different Endoscopic Approaches for Deep (Subserosal) Gastric Wall Biopsies: What Works? Gastrointest Endosc. 2006;63(5):AB233. - PubMed
-
- Sumiyama K, Rajan E. Endosocpic caps. Techniques in Gatrointestinal Endoscopy. 2006;8:28–32.
-
- Inoue H, Endo M, Takeshita K, Yoshino K, Muraoka Y, Yoneshima A new simplified technique of endoscopic esophageal mucosal resection using a cap-fitted panendoscope (EMRC) Surg Endosc. 1992;6:264–265. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
