

Risk factors for ARDS in patients receiving mechanical ventilation for > 48 h
- PMID: 18263691
- PMCID: PMC2628459
- DOI: 10.1378/chest.07-1121
Risk factors for ARDS in patients receiving mechanical ventilation for > 48 h
Abstract
Background: Low tidal volume (Vt) ventilation for ARDS is a well-accepted concept. However, controversy persists regarding the optimal ventilator settings for patients without ARDS receiving mechanical ventilation. This study tested the hypothesis that ventilator settings influence the development of new ARDS.
Methods: Retrospective analysis of patients from the Multi Parameter Intelligent Monitoring of Intensive Care-II project database who received mechanical ventilation for > or = 48 h between 2001 and 2005.
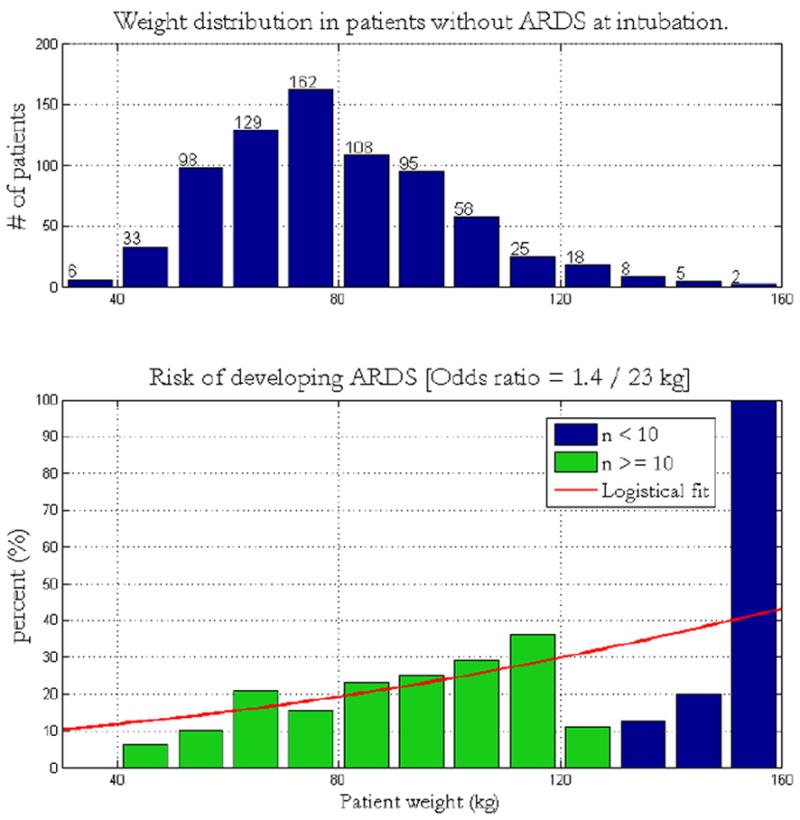
Results: A total of 2,583 patients required > 48 h of ventilation. Of 789 patients who did not have ARDS at hospital admission, ARDS developed in 152 patients (19%). Univariate analysis revealed high peak inspiratory pressure (odds ratio [OR], 1.53 per SD; 95% confidence interval [CI], 1.28 to 1.84), increasing positive end-expiratory pressure (OR, 1.35 per SD; 95% CI, 1.15 to 1.58), and Vt (OR, 1.36 per SD; 95% CI, 1.12 to 1.64) to be significant risk factors. Major nonventilator risk factors for ARDS included sepsis, low pH, elevated lactate, low albumin, transfusion of packed RBCs, transfusion of plasma, high net fluid balance, and low respiratory compliance. Multivariable logistic regression showed that peak pressure (OR, 1.31 per SD; 95% CI, 1.08 to 1.59), high net fluid balance (OR, 1.3 per SD; 95% CI, 1.09 to 1.56), transfusion of plasma (OR, 1.26 per SD; 95% CI, 1.07 to 1.49), sepsis (OR, 1.57; 95% CI, 1.00 to 2.45), and Vt (OR, 1.29 per SD; 95% CI, 1.02 to 1.52) were significantly associated with the development of ARDS.
Conclusions: The associations between the development of ARDS and clinical interventions, including high airway pressures, high Vt, positive fluid balance, and transfusion of blood products, suggests that ARDS may be a preventable complication in some cases.
Conflict of interest statement
Figures




References
-
- Esteban A, Anzueto A, Frutos F, et al. Characteristics and outcomes in adult patients receiving mechanical ventilation. J Am Med Assoc. 2002;287:345–355. - PubMed
-
- Amato MB, Barbas CS, Medeiros DM, et al. Effect of a protective-ventilation strategy on mortality in the acute respiratory distress syndrome. N Engl J Med. 1998;338:347–354. - PubMed
-
- Carlucci A, Richard JC, Wysocki M, et al. Noninvasive versus conventional mechanical ventilation. Am J Respir Crit Care Med. 2001;163(4):874–880. - PubMed
-
- The Acute Respiratory Distress Syndrome Network. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. 2000;342:1301–1308. - PubMed
-
- Gurkan OU, O’Donnell C, Brower R, et al. Differential effects of mechanical ventilatory strategy on lung injury and systemic organ inflammation in mice. Am J Physiol Lung Cell Mol Physiol. 2003 Sep;285(3):L710–718. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
