

Papillary microcarcinoma
- PMID: 18264828
- PMCID: PMC2323028
- DOI: 10.1007/s00268-007-9453-0
Papillary microcarcinoma
Abstract
Background: Papillary microcarcinoma (PMC) is increasing in incidence because of diagnosis by ultrasound-guided fine-needle aspiration cytology.
Methods: Between January 1966 and December 1995, we treated 6019 patients with papillary cancer; among them, 2070 patients with PMC were studied.
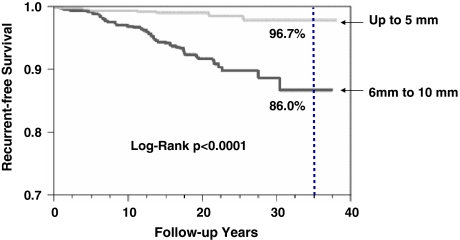
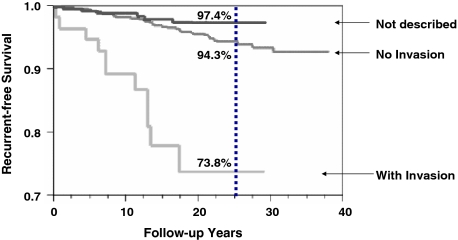
Results: PMC is essentially very similar to papillary cancer that is 11 mm or larger and has a very good prognosis. Smaller tumors and younger patients have a better prognosis. Among PMC, larger tumors (6-10 mm) recur in 14% at 35 years compared with 3.3% in patients with smaller tumors. Patients older than 55 years have recurrence in 40% at 30 years, with a worse prognosis than younger patients who have a recurrence rate of less than 10%. Extracapsular invasion by the primary tumor also has a higher recurrence rate. The majority of recurrences are in the neck. Therefore, annual ultrasound of the neck is effective for recurrence surveillance.
Conclusion: Papillary microcarcinoma is similar to larger papillary carcinomas with tumor characteristics and age-based recurrence rate that extends for many years, justifying long surveillance after surgery.
Figures








Similar articles
-
Routine Prophylactic Central Neck Dissection May Not Obviously Reduce Lateral Neck Recurrence for Papillary Thyroid Microcarcinoma.ORL J Otorhinolaryngol Relat Spec. 2019;81(2-3):73-81. doi: 10.1159/000497407. Epub 2019 Jun 12. ORL J Otorhinolaryngol Relat Spec. 2019. PMID: 31189172
-
Cancer recurrence in papillary thyroid microcarcinoma: a multivariate analysis on 231 patients with a 12-year follow-up.Minerva Endocrinol. 2013 Sep;38(3):269-79. Minerva Endocrinol. 2013. PMID: 24126547
-
Papillary thyroid microcarcinoma in Denmark 1996-2008: a national study of epidemiology and clinical significance.Thyroid. 2013 Sep;23(9):1159-64. doi: 10.1089/thy.2012.0595. Epub 2013 Aug 28. Thyroid. 2013. PMID: 23427917
-
[Papillary thyroid microcarcinoma].Sheng Wu Yi Xue Gong Cheng Xue Za Zhi. 2009 Oct;26(5):1167-70. Sheng Wu Yi Xue Gong Cheng Xue Za Zhi. 2009. PMID: 19947513 Review. Chinese.
-
Management of papillary microcarcinoma of the thyroid.S D Med. 2006 Oct;59(10):425-7. S D Med. 2006. PMID: 17124919 Review.
Cited by
-
Thyroid incidentalomas: epidemiology, risk stratification with ultrasound and workup.Eur Thyroid J. 2014 Sep;3(3):154-63. doi: 10.1159/000365289. Epub 2014 Sep 5. Eur Thyroid J. 2014. PMID: 25538897 Free PMC article. Review.
-
Papillary thyroid microcarcinoma with lung metastases: a case report and review of the literature.Thyroid Res. 2021 Jun 11;14(1):15. doi: 10.1186/s13044-021-00106-0. Thyroid Res. 2021. PMID: 34116701 Free PMC article.
-
The Extent of Surgery for Papillary Thyroid Microcarcinoma: The Controversy Continues.World J Surg. 2017 Jan;41(1):136-137. doi: 10.1007/s00268-016-3726-4. World J Surg. 2017. PMID: 27695929 No abstract available.
-
Differences in the Form of Presentation between Papillary Microcarcinomas and Papillary Carcinomas of Larger Size.J Thyroid Res. 2010 Dec 14;2011:639156. doi: 10.4061/2011/639156. J Thyroid Res. 2010. PMID: 21209704 Free PMC article.
-
RETRACTED ARTICLE: Thyroid nodules update in diagnosis and management.Clin Diabetes Endocrinol. 2015 Sep 18;1:11. doi: 10.1186/s40842-015-0011-7. eCollection 2015. Clin Diabetes Endocrinol. 2015. Retraction in: Clin Diabetes Endocrinol. 2016 Apr 14;2:10. doi: 10.1186/s40842-016-0025-9. PMID: 28702230 Free PMC article. Retracted.
References
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1089/105072503321669875', 'is_inner': False, 'url': 'https://doi.org/10.1089/105072503321669875'}, {'type': 'PubMed', 'value': '12804106', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/12804106/'}]}
- Ito Y, Uruno T, Nakano K et al (2003) An observation trial without surgical treatment in patients with papillary microcarcinoma of the thyroid. Thyroid 13:381–387 - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1097/01.rlu.0000257272.90126.3d', 'is_inner': False, 'url': 'https://doi.org/10.1097/01.rlu.0000257272.90126.3d'}, {'type': 'PubMed', 'value': '17413573', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/17413573/'}]}
- Kucuk NO, Tari P, Tokmak E et al (2007) Treatment for microcarcinoma of the thyroid—clinical experience. Clin Nucl Med 32:279–281 - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1016/j.ejso.2006.07.001', 'is_inner': False, 'url': 'https://doi.org/10.1016/j.ejso.2006.07.001'}, {'type': 'PubMed', 'value': '16872798', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/16872798/'}]}
- Pelizzo MR, Boschin IM, Toniato A et al (2006) Papillary thyroid microcarcinoma (PTMC): prognostic factors, management and outcome in 403 patients. Eur J Surg Oncol 32:1144–1148 - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1002/1097-0142(197509)36:3<1095::AID-CNCR2820360338>3.0.CO;2-9', 'is_inner': False, 'url': 'https://doi.org/10.1002/1097-0142(197509)36:3<1095::aid-cncr2820360338>3.0.co;2-9'}, {'type': 'PubMed', 'value': '1182663', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/1182663/'}]}
- Fukunaga FH, Yatani R (1975) Geographic pathology of occult thyroid carcinomas. Cancer 36:1095–1099 - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1002/1097-0142(19841015)54:8<1625::AID-CNCR2820540825>3.0.CO;2-0', 'is_inner': False, 'url': 'https://doi.org/10.1002/1097-0142(19841015)54:8<1625::aid-cncr2820540825>3.0.co;2-0'}, {'type': 'PubMed', 'value': '6478402', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/6478402/'}]}
- Grant S, Luttrell B, Reeve T et al (1984) Thyroglobulin may be undetectable in the serum of patients with metastatic disease secondary to differentiated thyroid carcinoma. Follow-up of differentiated thyroid carcinoma. Cancer 54:1625–1628 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
