

Biological augmentation of rotator cuff tendon repair
- PMID: 18264850
- PMCID: PMC2505220
- DOI: 10.1007/s11999-007-0112-4
Biological augmentation of rotator cuff tendon repair
Abstract
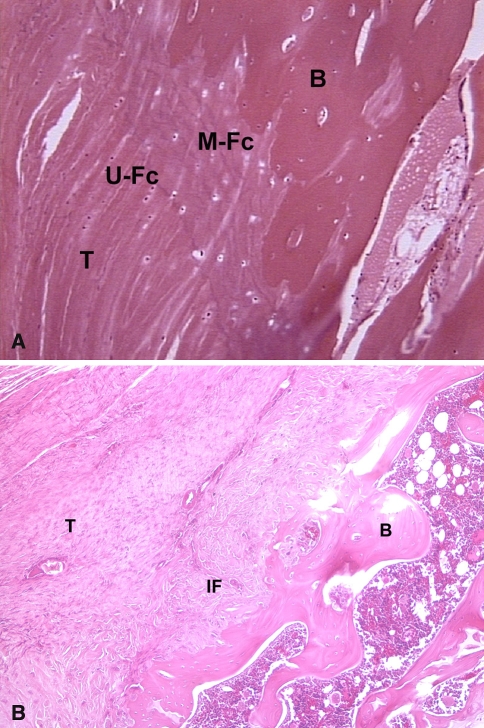
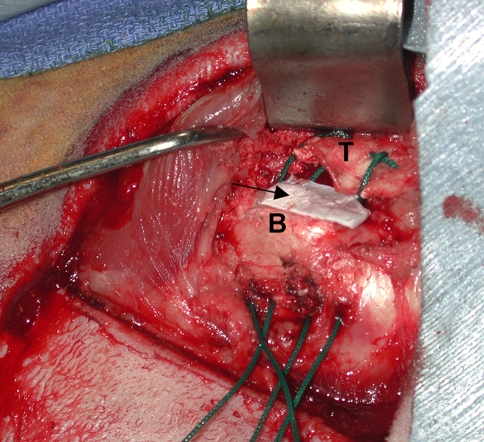
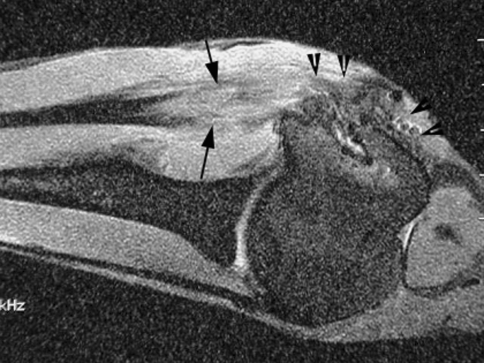
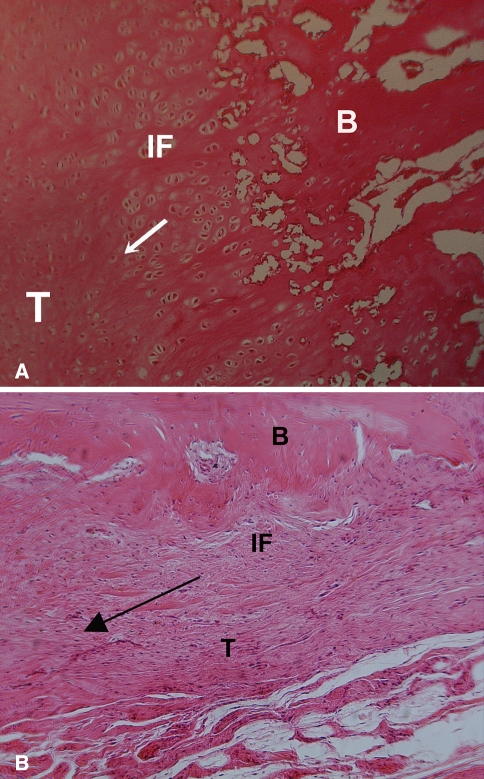
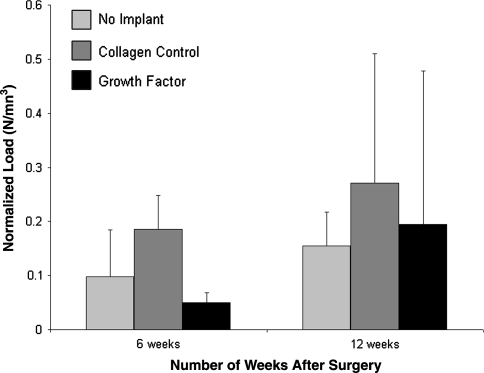
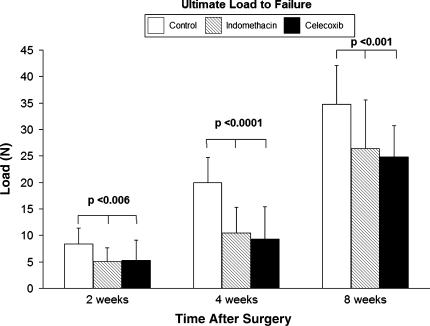
A histologically normal insertion site does not regenerate following rotator cuff tendon-to-bone repair, which is likely due to abnormal or insufficient gene expression and/or cell differentiation at the repair site. Techniques to manipulate the biologic events following tendon repair may improve healing. We used a sheep infraspinatus repair model to evaluate the effect of osteoinductive growth factors and BMP-12 on tendon-to-bone healing. Magnetic resonance imaging and histology showed increased formation of new bone and fibrocartilage at the healing tendon attachment site in the treated animals, and biomechanical testing showed improved load-to-failure. Other techniques with potential to augment repair site biology include use of platelets isolated from autologous blood to deliver growth factors to a tendon repair site. Modalities that improve local vascularity, such as pulsed ultrasound, have the potential to augment rotator cuff healing. Important information about the biology of tendon healing can also be gained from studies of substances that inhibit healing, such as nicotine and antiinflammatory medications. Future approaches may include the use of stem cells and transcription factors to induce formation of the native tendon-bone insertion site after rotator cuff repair surgery.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
