

Comparison of provincial prescription drug plans and the impact on patients' annual drug expenditures
- PMID: 18268266
- PMCID: PMC2228358
- DOI: 10.1503/cmaj.070587
Comparison of provincial prescription drug plans and the impact on patients' annual drug expenditures
Abstract
Background: Reimbursement for outpatient prescription drugs is not mandated by the Canada Health Act or any other federal legislation. Provincial governments independently establish reimbursement plans. We sought to describe variations in publicly funded provincial drug plans across Canada and to examine the impact of this variation on patients' annual expenditures.
Methods: We collected information, accurate to December 2006, about publicly funded prescription drug plans from all 10 Canadian provinces. Using clinical scenarios, we calculated the impact of provincial cost-sharing strategies on individual annual drug expenditures for 3 categories of patients with different levels of income and 2 levels of annual prescription burden ($260 and $1000).
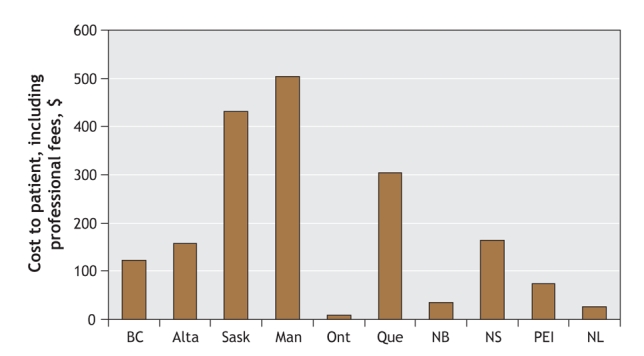
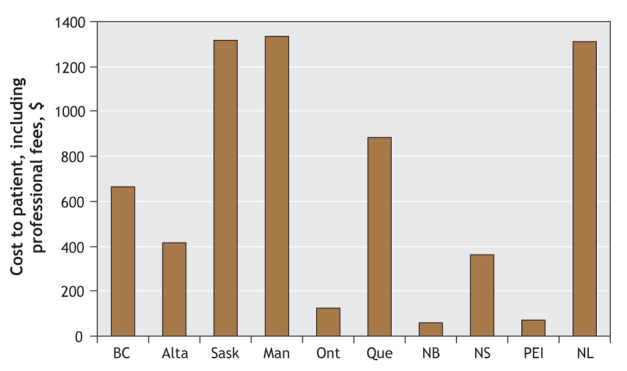
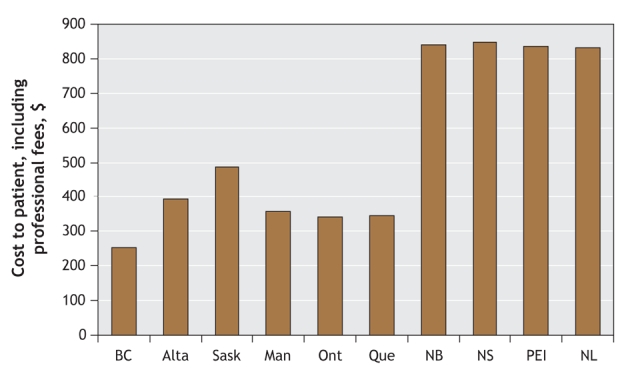
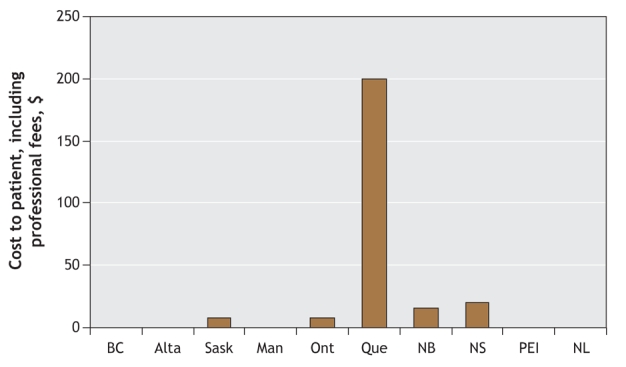
Results: We found that eligibility criteria and cost-sharing details of the publicly funded prescription drug plans differed markedly across Canada, as did the personal financial burden due to prescription drug costs. Seniors pay 35% or less of their prescription costs in 2 provinces, but elsewhere they may pay as much as 100%. With few exceptions, nonseniors pay more than 35% of their prescription costs in every province. Most social assistance recipients pay 35% or less of their prescription costs in 5 provinces and pay no costs in the other 5. In an example of a patient with congestive heart failure, his out-of-pocket costs for a prescription burden of $1283 varied between $74 and $1332 across the provinces.
Interpretation: Considerable interprovincial variation in publicly funded prescription drug plans results in substantial variation in annual expenditures by Canadians with identical prescription burdens. A revised pharmaceutical strategy might reduce these major inequities.
Figures
References
-
- Drug expenditure in Canada 1985 to 2005: National Health Expenditure Database. Ottawa: Canadian Institute for Health Information; 2006. Available: http://dsp-psd.pwgsc.gc.ca/Collection/H115-27-2005E.pdf (accessed 2007 Dec 10).
-
- Tamblyn R, Laprise R, Hanley JA, et al. Adverse events associated with prescription drug cost-sharing among poor and elderly persons. JAMA 2001;285:421-9. - PubMed
-
- Soumerai SB, McLaughlin TJ, Ross-Degnan D, et al. Effects of a limit on Medicaid drug-reimbursement benefits on the use of psychotropic agents and acute mental health services by patient with schizophrenia. N Engl J Med 1994;331:650-5. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical