

Restrictive access to clopidogrel and mortality following coronary stent implantation
- PMID: 18268267
- PMCID: PMC2228353
- DOI: 10.1503/cmaj.070586
Restrictive access to clopidogrel and mortality following coronary stent implantation
Abstract
Background: In Canada, access to clopidogrel is restricted by most provincial drug insurance plans in order to contain costs. Until April 2007, the Régie de l'assurance maladie du Québec (RAMQ) Prescription Drug Insurance Plan reviewed special access forms before approving reimbursement for clopidogrel prescriptions. We investigated the impact of this restrictive process on patient's filling of prescriptions and on all-cause mortality following coronary stenting.
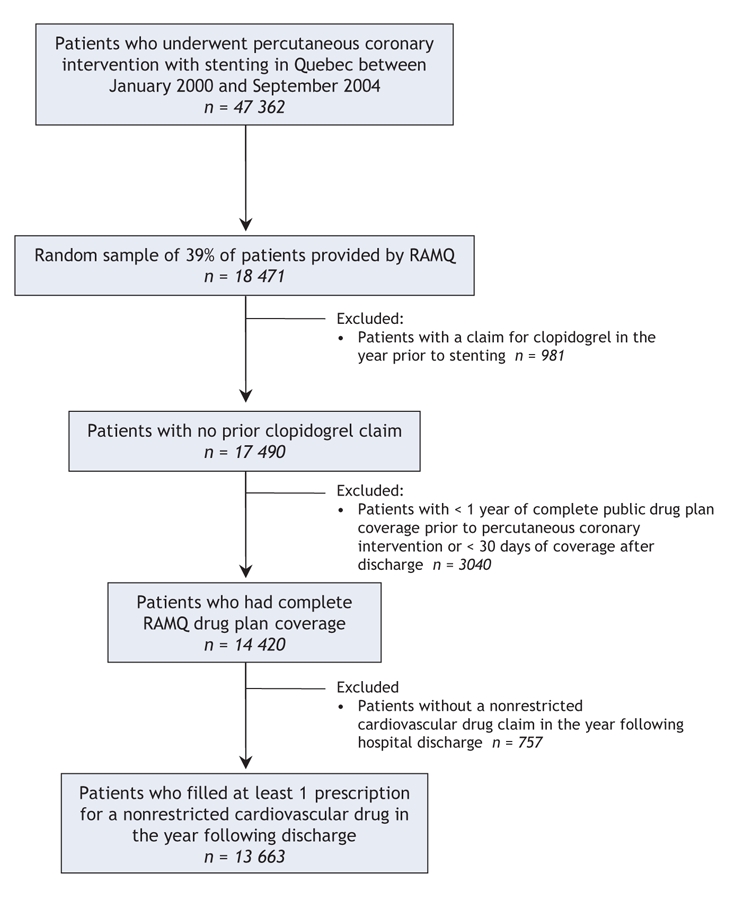
Methods: We analyzed prescriptions filled and all-cause mortality in the year following a percutaneous coronary intervention among patients who underwent stent implantation between January 2000 and September 2004. We obtained administrative data from the RAMQ databases. We included patients who filled at least 1 prescription for a nonrestricted cardiovascular drug after hospital discharge. We used Cox proportional models to compare mortality rates as a function of delayed or absent outpatient clopidogrel therapy.
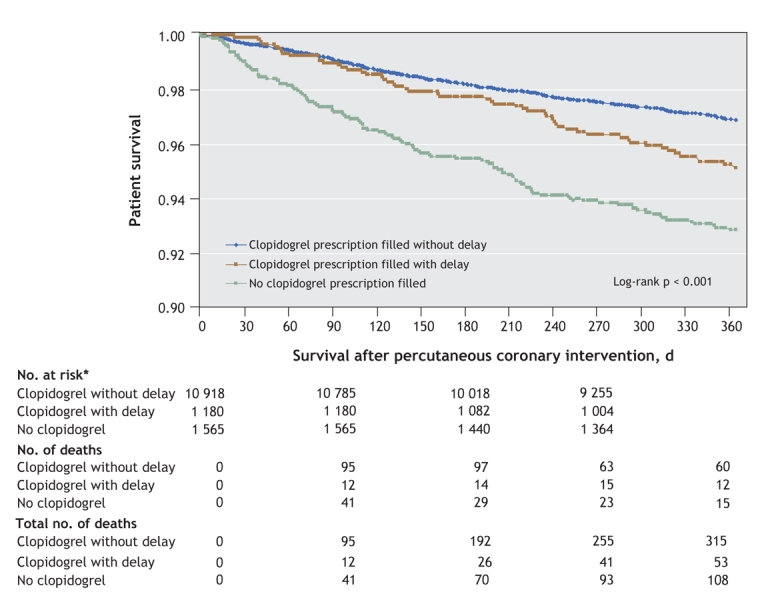
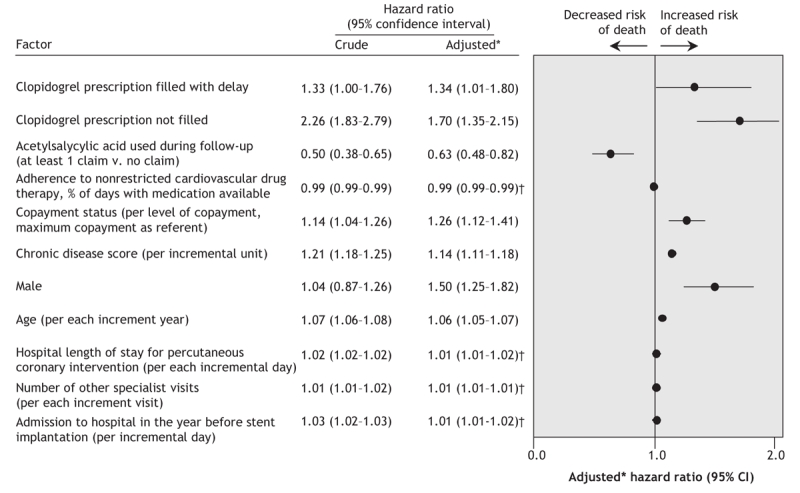
Results: Of 13,663 patients, 1571 (11.5%) did not fill any clopidogrel prescription despite filling at least 1 nonrestricted cardiovascular drug prescription after a percutaneous coronary intervention, and 1174 (8.6%) patients filled their clopidogrel prescription with a delay of at least 1 day (median delay 5 days) after filling the nonrestricted cardiovascular drug prescription. After controlling for pertinent covariables, not filling a clopidogrel prescription (hazard ratio [HR] 1.70, 95% confidence interval [CI] 1.35-2.15) and filling with a delay (HR 1.34, 95% CI 1.01-1.80) were associated with a significant increase in all-cause mortality.
Interpretation: Restricted access to clopidogrel was associated with about 20% of patients either not receiving clopidogrel or receiving therapy after a delay. Delay or absence of clopidogrel therapy increased the risk of all-cause mortality after percutaneous coronary intervention with stenting.
Figures
Comment in
-
Mortality benefit from unrestricted access to clopidogrel: too good to be true?CMAJ. 2008 Feb 12;178(4):425-7. doi: 10.1503/cmaj.071592. CMAJ. 2008. PMID: 18268269 Free PMC article. Review. No abstract available.
References
-
- Faulkner LA, Schauffler HH. The effect of health insurance coverage on the appropriate use of recommended clinical preventive services. Am J Prev Med 1997;13:453-8. - PubMed
-
- Burroughs VJ. Why worry about restricting access to medicines in Medicaid? Am J Manag Care. 2005;11 Spec No:SP4-5. - PubMed
-
- Régie de l'assurance maladie du Quebec: service de l'information aux professionnels. Liste de médicaments. 13th edition. Quebec: Régie de l'assurance maladie; 2006. Available: www.ramq.gouv.qc.ca/fr/professionnels/listmed/lm_tdmf_ajour.shtml#ahfs (accessed 2008 Jan 11).
-
- Cutlip DE, Baim DS, Ho KK, et al. Stent thrombosis in the modern era: a pooled analysis of multicenter coronary stent clinical trials. Circulation 2001;103:1967-71. - PubMed
-
- Bertrand ME, Legrand V, Boland J, et al. Randomized multicenter comparison of conventional anticoagulation versus antiplatelet therapy in unplanned and elective coronary stenting. The full anticoagulation versus aspirin and ticlopidine (fantastic) study. Circulation 1998;98:1597-603. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous