

Posterior reversible encephalopathy syndrome after solid organ transplantation
- PMID: 18272559
- PMCID: PMC8128592
- DOI: 10.3174/ajnr.A0960
Posterior reversible encephalopathy syndrome after solid organ transplantation
Abstract
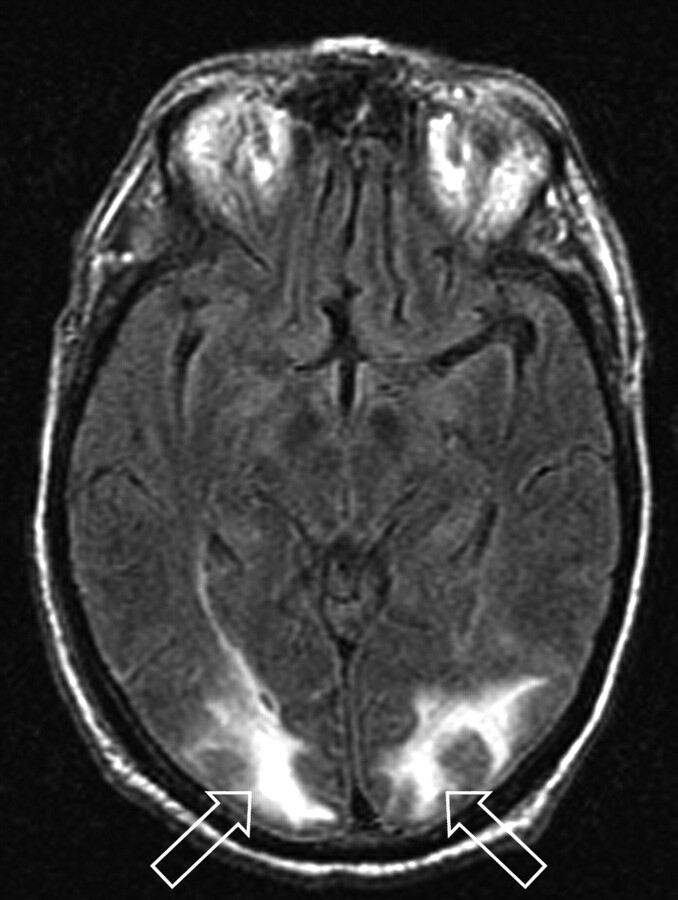
Background and purpose: Posterior reversible encephalopathy syndrome (PRES) is known to occur after solid organ transplantation (SOT), potentially associated with cyclosporine and tacrolimus. In this study, we assess the frequency and clinical and imaging characteristics of PRES after SOT.
Materials and methods: We identified 27 patients (13 men and 14 women; age range, 22-72 years) who developed PRES after SOT. Features noted included SOT subtype, incidence and timing of PRES, infection and rejection, mean arterial pressure (MAP), and toxicity brain edema.
Results: PRES developed in 21 (0.49%) of 4222 patients who underwent transplantation within the study period (no significant difference among SOT subtypes). Transplantation was performed in 5 patients before the study period, and 1 patient underwent transplantation elsewhere. In consideration of all 27 patients, PRES typically developed in the first 2 months in patients who had SOT of the liver (9 of 10 patients) and was associated with cytomegalovirus (CMV), mild rejection, or systemic bacterial infection. PRES also typically developed after 1 year in patients who had SOT of the kidney (8 of 9 patients) and was associated with moderate rejection or bacterial infection. Toxicity MAP was significantly lower (P < .001) in liver transplants (average MAP, 104.8 +/- 16 mm Hg) compared with that in kidney transplants (average MAP, 143 +/- 20 mm Hg). Toxicity brain edema was significantly greater (P < .001) in patients who had liver transplants and developed PRES compared with patients who had undergone kidney transplants despite severe hypertension in those who had the kidney transplants.
Conclusion: Patients who had undergone SOTs have a similar low incidence of developing PRES. Differences between those who have had liver and kidney transplants included time after transplant, toxicity MAP, and PRES vasogenic edema noted at presentation. In patients who have undergone kidney transplants, severely elevated MAP was associated with reduced, not greater, brain edema.
Figures

References
-
- Bartynski WS, Grabb BC, Zeigler Z, et al. Watershed imaging features and clinical vascular injury in cyclosporin A neurotoxicity. J Comput Assist Tomogr 1997;21:872–80 - PubMed
-
- Hinchey J, Chaves C, Appignani B, et al. A reversible posterior leukoencephalopathy syndrome. N Engl J Med 1996;334:494–500 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical