

Peripherally acting mu-opioid receptor agonist attenuates neuropathic pain in rats after L5 spinal nerve injury
- PMID: 18276075
- PMCID: PMC2805197
- DOI: 10.1016/j.pain.2008.01.004
Peripherally acting mu-opioid receptor agonist attenuates neuropathic pain in rats after L5 spinal nerve injury
Abstract
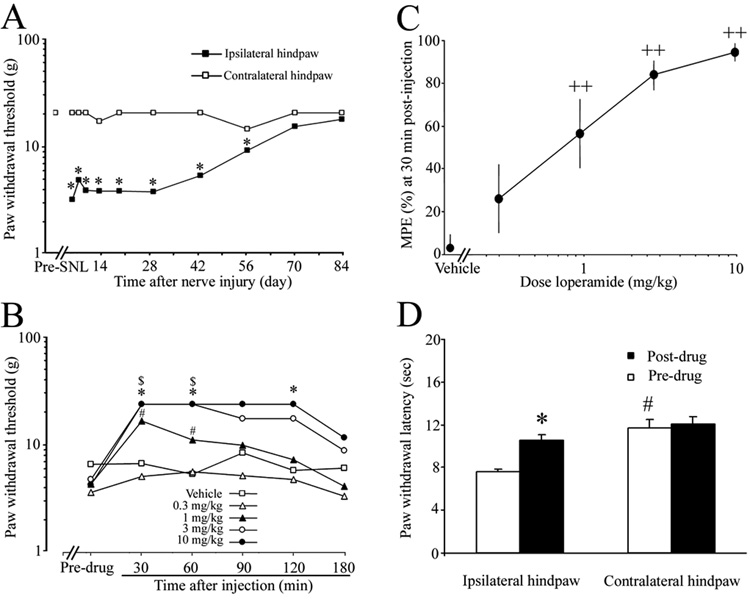
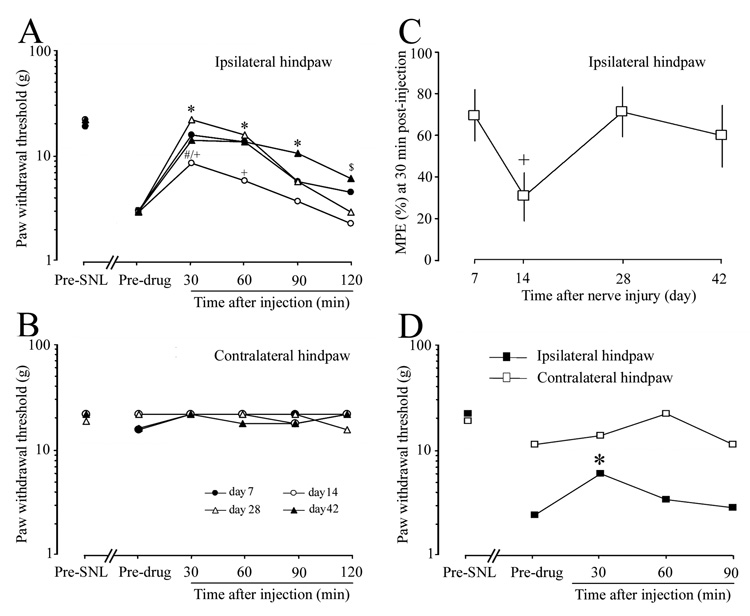
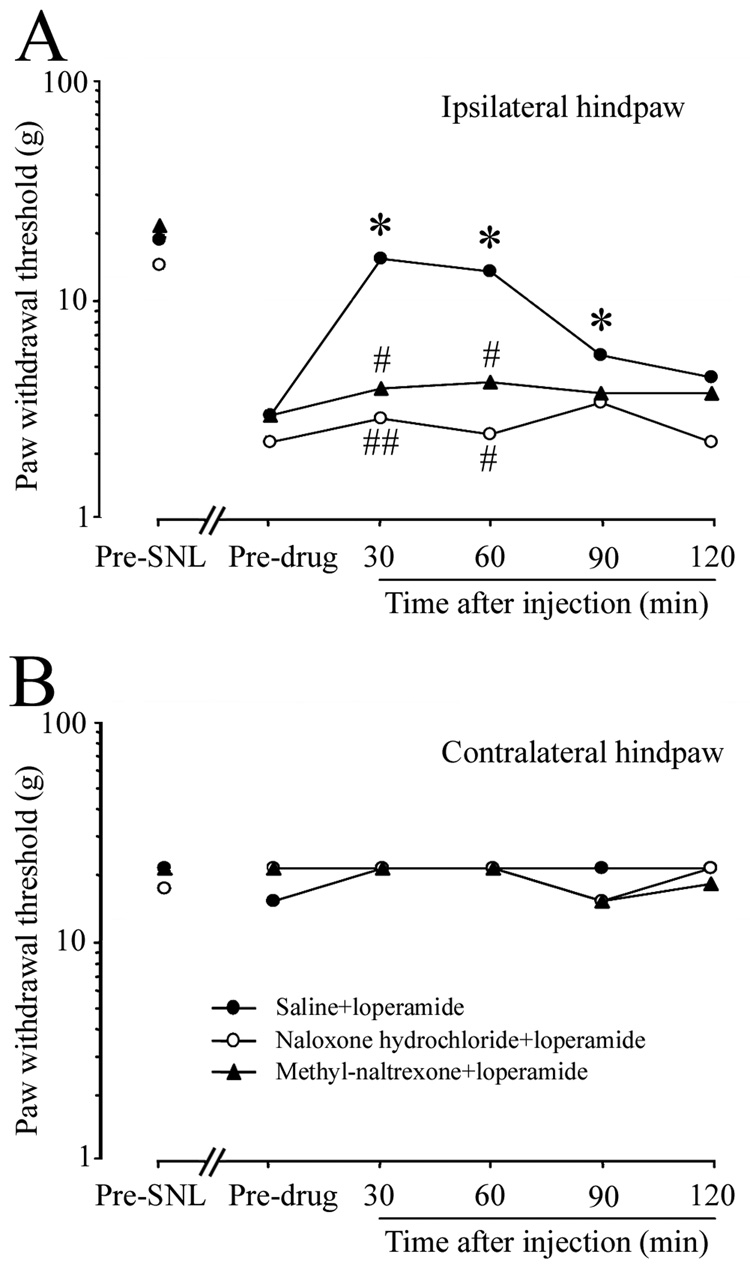
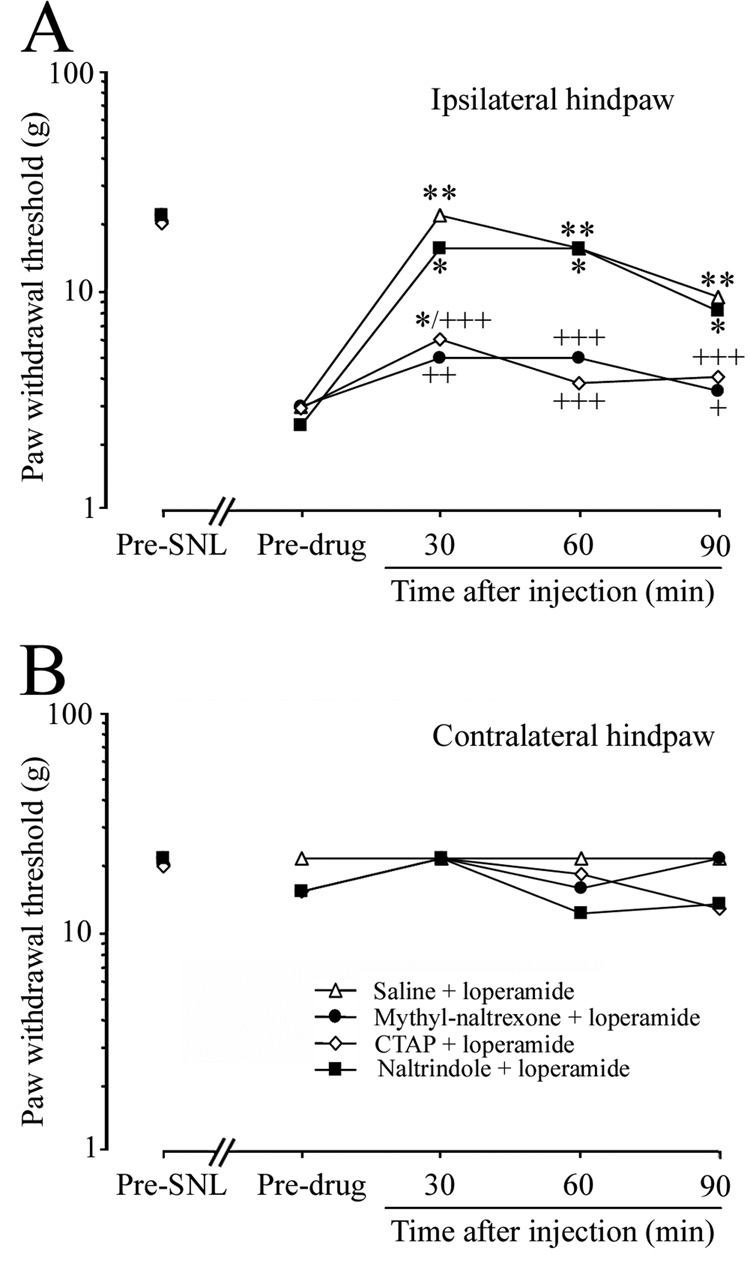
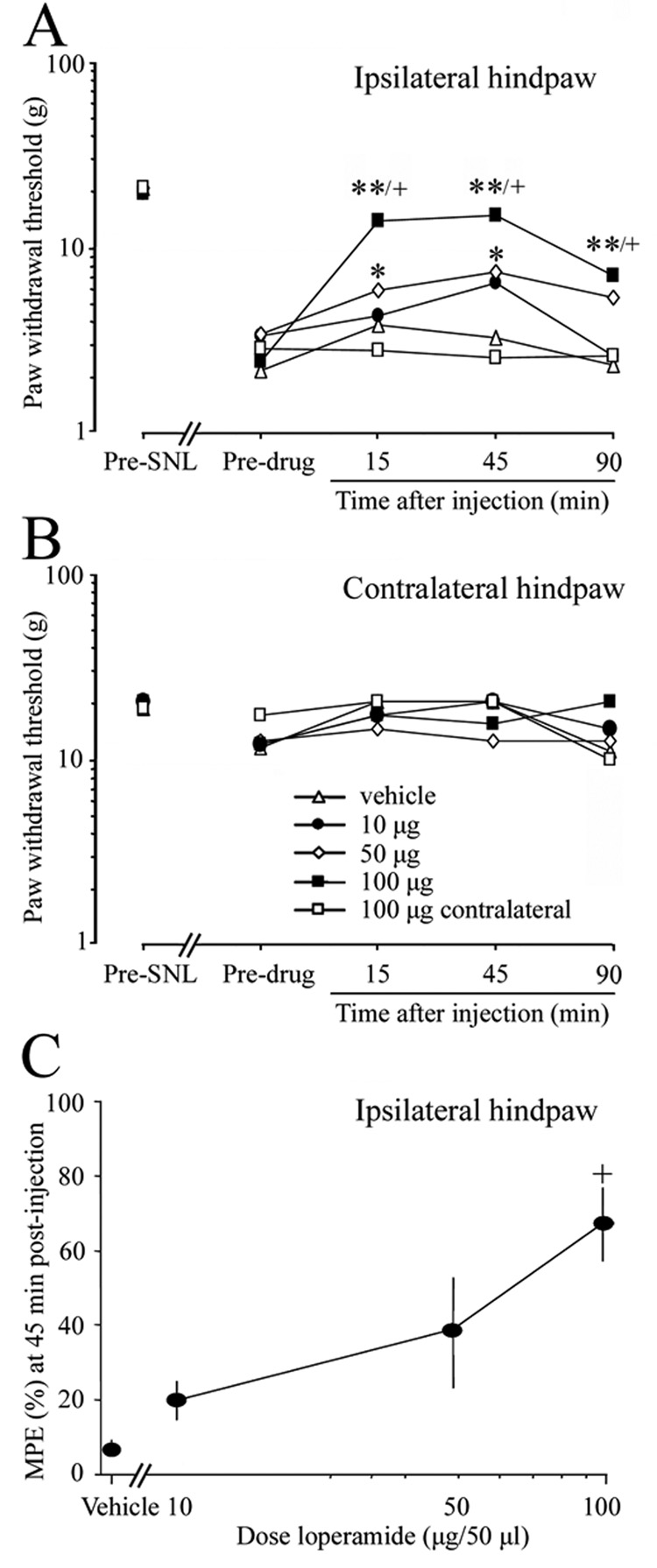
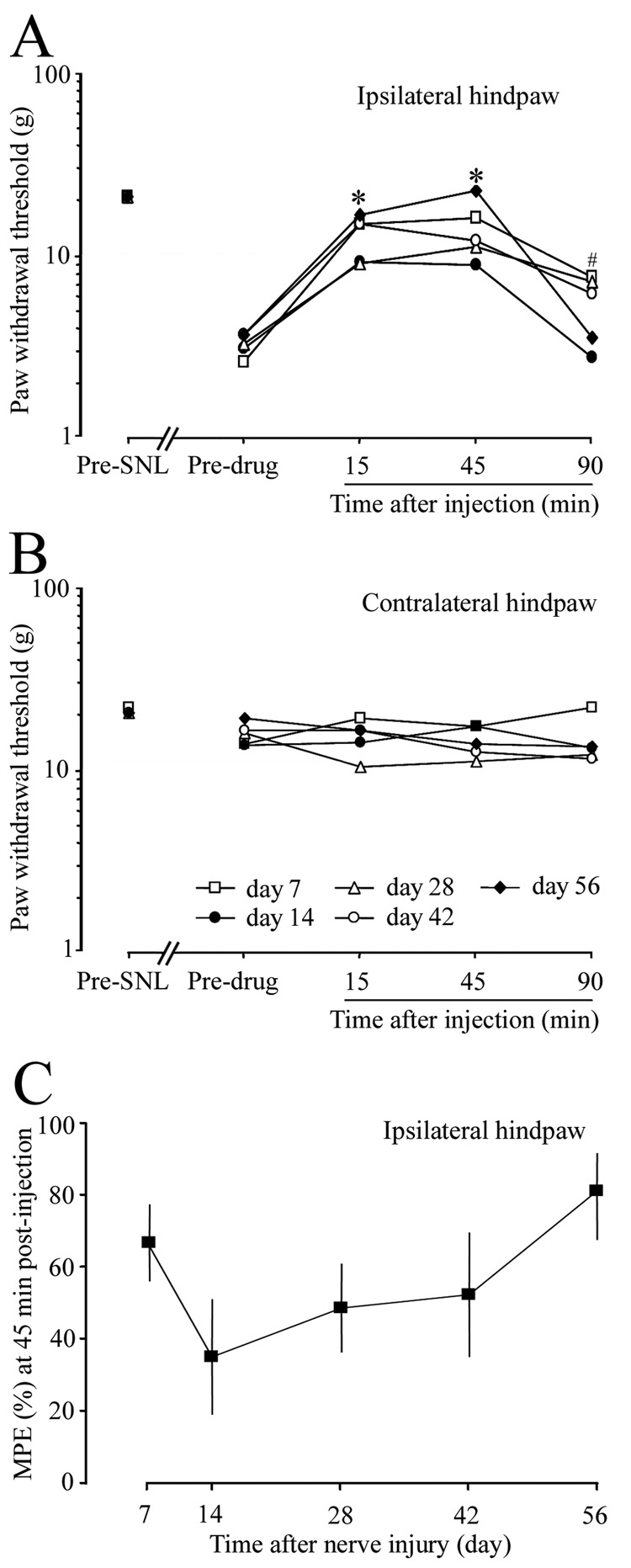
Studies in experimental models and controlled patient trials indicate that opioids are effective in managing neuropathic pain. However, side effects secondary to their central nervous system actions present barriers to their clinical use. Therefore, we examined whether activation of the peripheral mu-opioid receptors (MORs) could effectively alleviate neuropathic pain in rats after L5 spinal nerve ligation (SNL). Systemic loperamide hydrochloride (0.3-10 mg/kg, s.c.), a peripherally acting MOR-preferring agonist, dose-dependently reversed the mechanical allodynia at day 7 post-SNL. This anti-allodynic effect produced by systemic loperamide (1.5mg/kg, s.c.) was blocked by systemic pretreatment with either naloxone hydrochloride (10 mg/kg, i.p.) or methyl-naltrexone (5 mg/kg, i.p.), a peripherally acting MOR-preferring antagonist. It was also blocked by ipsilateral intraplantar pretreatment with methyl-naltrexone (43.5 microg/50 microl) and the highly selective MOR antagonist CTAP (5.5 microg/50 microl). However, this anti-allodynic effect of systemic loperamide was not blocked by intraplantar pretreatment with the delta-opioid receptor antagonist naltrindole hydrochloride (45.1 microg/50 microl). The anti-allodynic potency of systemic loperamide varied with time after nerve injury, with similar potency at days 7, 28, and 42 post-SNL, but reduced potency at day 14 post-SNL. Ipsilateral intraplantar injection of loperamide also dose-dependently (10-100 microg/50 microl) reversed mechanical allodynia on day 7 post-SNL. We suggest that loperamide can effectively attenuate neuropathic pain, primarily through activation of peripheral MORs in local tissue. Therefore, peripherally acting MOR agonists may represent a promising therapeutic approach for alleviating neuropathic pain.
Figures
References
-
- Andreev N, Urban L, Dray A. Opioids suppress spontaneous activity of polymodal nociceptors in rat paw skin induced by ultraviolet irradiation. Neuroscience. 1994;58:793–798. - PubMed
-
- Baker AK, Meert TF. Functional effects of systemically administered agonists andantagonists of mu, delta, and kappa opioid receptor subtypes on body temperature in mice. J Pharmacol Exp Ther. 2002;302:1253–1264. - PubMed
-
- Bian D, Nichols ML, Ossipov MH, Lai J, Porreca F. Characterization of the antiallodynic efficacy of morphine in a model of neuropathic pain in rats. Neuroreport. 1995;6:1981–1984. - PubMed
-
- Chaplan SR, Bach FW, Pogrel JW, Chung JM, Yaksh TL. Quantitative assessment of tactile allodynia in the rat paw. J Neurosci Meth. 1994;53:55–63. - PubMed
-
- Chung JM, Chung K. Importance of hyperexcitability of DRG neurons in neuropathic pain. Pain Pract. 2002;2:87–97. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
