

Prevalence and treatment of isolated and concurrent hypertension and hypercholesterolaemia in the United Kingdom
- PMID: 18279464
- PMCID: PMC2432490
- DOI: 10.1111/j.1365-2125.2007.03072.x
Prevalence and treatment of isolated and concurrent hypertension and hypercholesterolaemia in the United Kingdom
Abstract
What is already known about this subject: The 1998 and 2003 Health Survey for England revealed a high prevalence of hypertension and hypercholesterolaemia in the population of England. Major changes in the reimbursement of primary care for the management of both hypertension and hypercholesterolaemia have occurred in the UK.
What this study adds: Using a GP database we have examined the proportion of subjects diagnosed and treated for hypertension and hypercholesterolaemia over time. To examine the true population rates and primary care data we compared the results of the Health survey for England in both 1998 and 2003 with the recorded data on GP computers. Despite current guidelines, many patients with hypertension and/or hypercholesterolaemia are under-treated and, even amongst those who are treated, many do not achieve their blood pressure and/or lipid targets. Although treatment rates in the UK have improved recently, particularly for lipid-lowering therapies, they remain suboptimal. AIMS To determine the prevalence and treatment of hypertension, dyslipidaemia and both together in the UK between 1998 and 2006.
Methods: We used The Health Improvement Network (THIN) a general practice-based database from 1998 to 2006 and we compared the 1998 and 2003 data to that taken from the Health Survey for England (HSE) in 1998 and 2003.
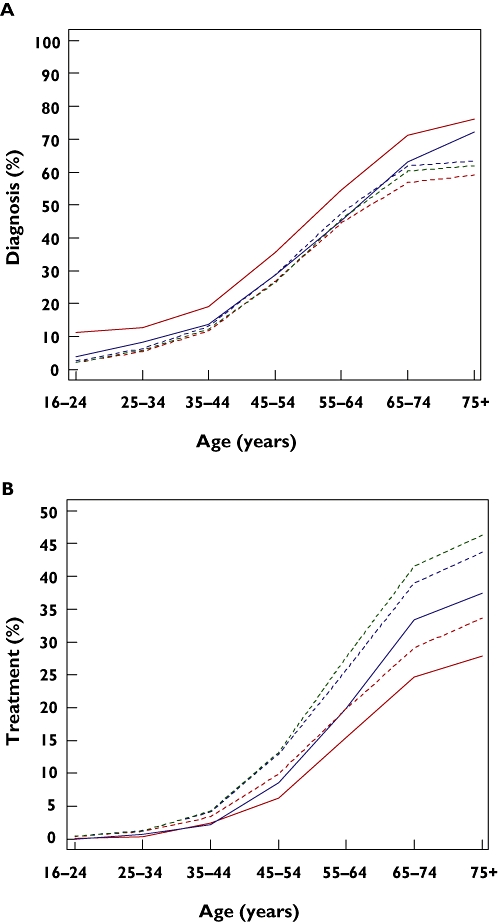
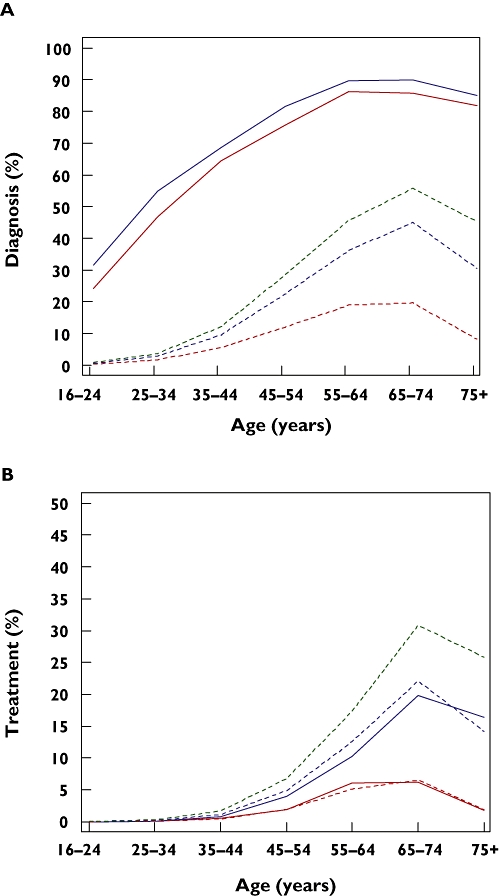
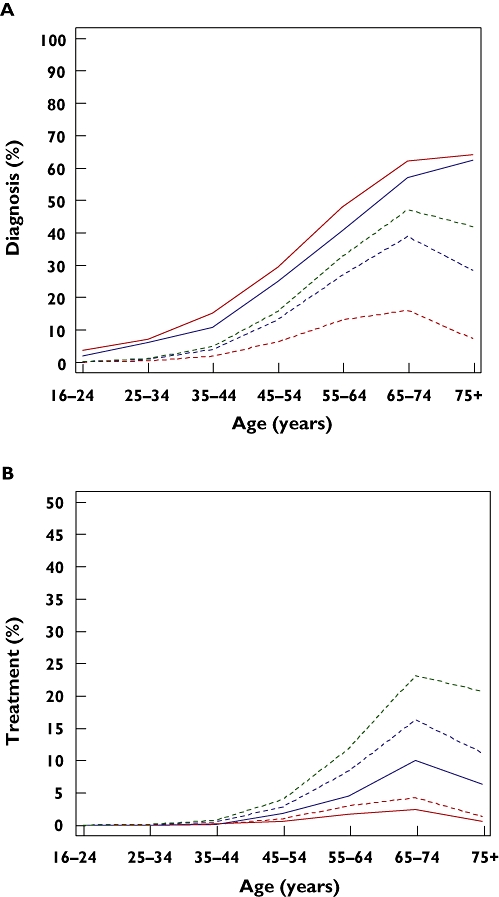
Results: The prevalence (treatment) of hypertension was 25.3% (11.4%) in 1998, 27.8% (15.1%) in 2003 and 26.9% (16.2%) in 2006 in THIN. In HSE it was 37.3% (9.6%) in 1998 and 32.9% (13.8%) in 2003. For dyslipidaemia the figures were 8.6% (1.9%), 18.5% (6.5%) and 24.4% (9.8%) for THIN and 67.8% (2.3%) and 74.9% (7.0%) for HSE. Concurrent hypertension and dyslipidaemia in THIN increased from 5.5% (1.1%) in 1998 to 13.5% (4.5%) in 2003 and 17.4% (7.1%) in 2006. The prevalence of both conditions was 30.6% (0.7%) in HSE in 1998 and 28.7% (3.1%) in 2003.
Conclusions: There has been a progressive improvement in the detection and treatment of hypertension, dyslipidaemia and both conditions together between 1998 and 2006. However, much still needs to be done to improve the diagnosis and treatment of hypertension, hypercholesterolaemia and concurrent hypertension and hypercholesterolaemia in the United Kingdom.
Figures
References
-
- Rayner M, Peterson S for the British Heart Foundation Health Promotion Research Group. European Cardiovascular Disease Statistics. 2000. Oxford: British Heart Foundation Health Promotion Research Group, Department of Public Health, University of Oxford, Institute of Health Sciences; 2000.
-
- De Backer G, Ambrosioni E, Borch-Johnsen K, Brotons C, Cifkova R, Dallongeville J, Ebrahim S, Faergeman O, Graham I, Mancia G, Manger Cats V, Orth-Gomér K, Perk J, Pyörälä K, Rodicio JL, Sans S, Sansoy V, Sechtem U, Silber S, Thomsen T, Wood D. European guidelines on cardiovascular disease prevention in clinical practice. Third Joint Task Force of European and Other Societies on Cardiovascular Disease Prevention in Clinical Practice. Eur Heart J. 2003;24:1601–10. - PubMed
-
- Ezzati M, Lopez AD, Rodgers A, Vander Hoorn S, Murray CJ. Selected major risk factors and global and regional burden of disease. Lancet. 2002;360:1347–60. - PubMed
-
- Kannel WB. Risk stratification in hypertension: new insights from the Framingham Study. Am J Hypertens. 2000;13(1 Pt 2):3S–10S. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
