

Multiple-dose activated charcoal in acute self-poisoning: a randomised controlled trial
- PMID: 18280328
- PMCID: PMC2430417
- DOI: 10.1016/S0140-6736(08)60270-6
Multiple-dose activated charcoal in acute self-poisoning: a randomised controlled trial
Abstract
Background: The case-fatality for intentional self-poisoning in the rural developing world is 10-50-fold higher than that in industrialised countries, mostly because of the use of highly toxic pesticides and plants. We therefore aimed to assess whether routine treatment with multiple-dose activated charcoal, to interrupt enterovascular or enterohepatic circulations, offers benefit compared with no charcoal in such an environment.
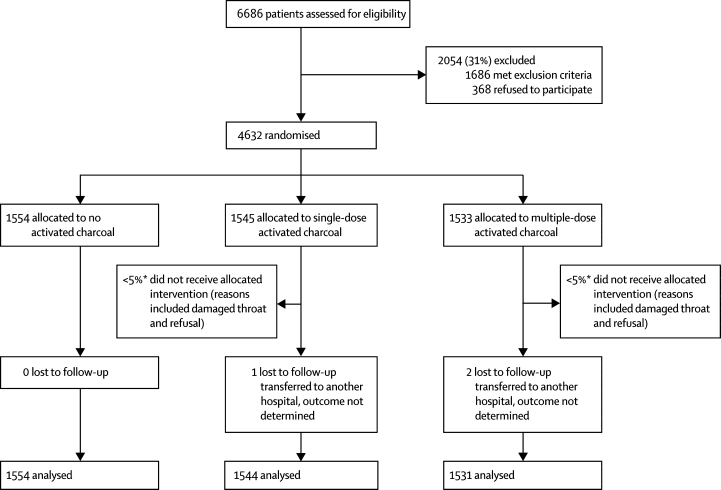
Methods: We did an open-label, parallel group, randomised, controlled trial of six 50 g doses of activated charcoal at 4-h intervals versus no charcoal versus one 50 g dose of activated charcoal in three Sri Lankan hospitals. 4632 patients were randomised to receive no charcoal (n=1554), one dose of charcoal (n=1545), or six doses of charcoal (n=1533); outcomes were available for 4629 patients. 2338 (51%) individuals had ingested pesticides, whereas 1647 (36%) had ingested yellow oleander (Thevetia peruviana) seeds. Mortality was the primary outcome measure. Analysis was by intention to treat. The trial is registered with controlled-trials.com as ISRCTN02920054.
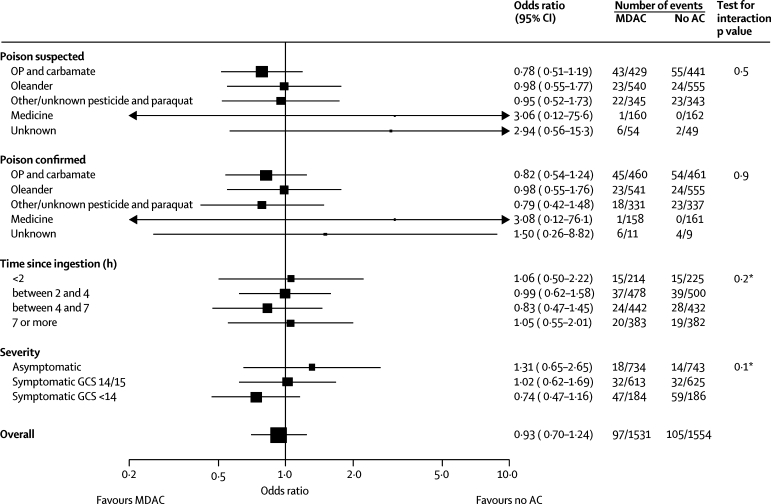
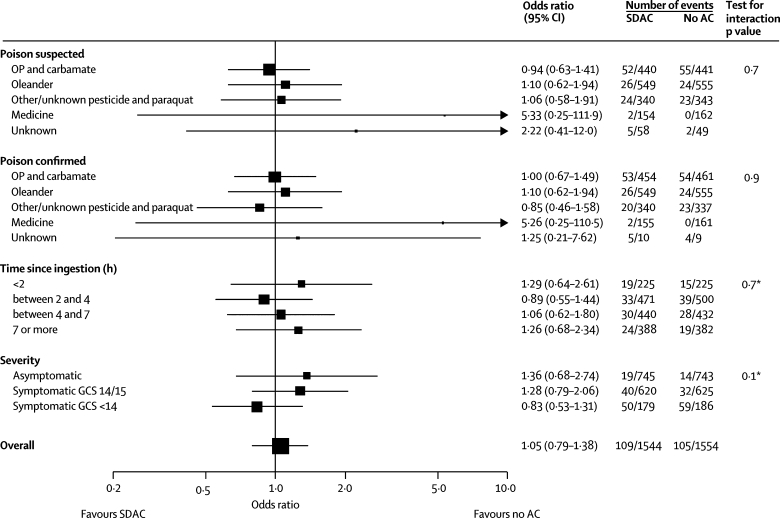
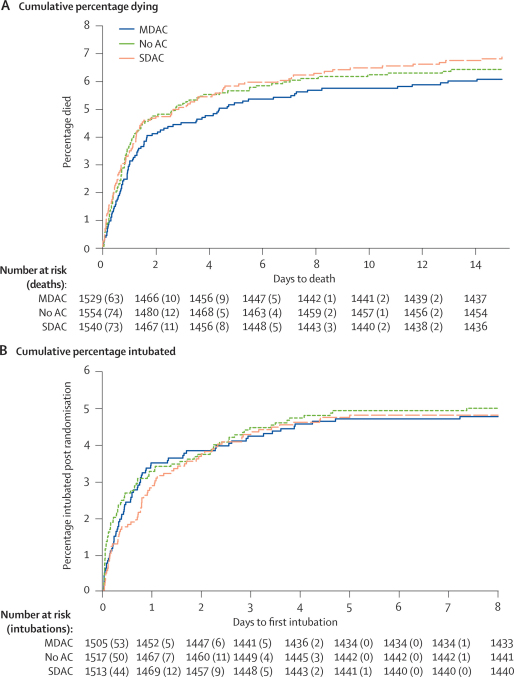
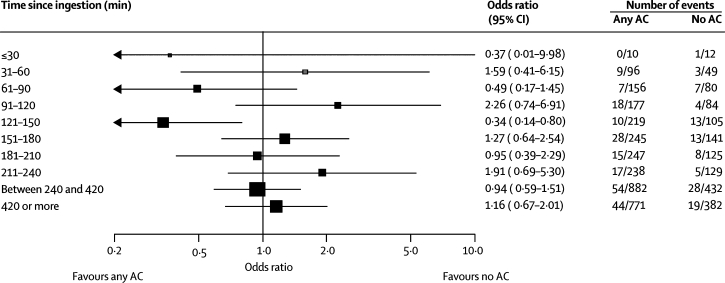
Findings: Mortality did not differ between the groups. 97 (6.3%) of 1531 participants in the multiple-dose group died, compared with 105 (6.8%) of 1554 in the no charcoal group (adjusted odds ratio 0.96, 95% CI 0.70-1.33). No differences were noted for patients who took particular poisons, were severely ill on admission, or who presented early.
Interpretation: We cannot recommend the routine use of multiple-dose activated charcoal in rural Asia Pacific; although further studies of early charcoal administration might be useful, effective affordable treatments are urgently needed.
Figures
Comment in
-
Is this the epitaph for multiple-dose activated charcoal?Lancet. 2008 Feb 16;371(9612):538-9. doi: 10.1016/S0140-6736(08)60248-2. Lancet. 2008. PMID: 18280313 No abstract available.
References
-
- Shannon MW, Haddad LM. The emergency management of poisoning. In: Haddad LM, Shannon MW, Winchester JF, editors. Clinical management of poisoning and drug overdose. 3rd edn. WBSaunders; Philadelphia: 1998. pp. 2–31.
-
- Keyes DC, Dart RC. Initial diagnosis and treatment of the poisoned patient. In: Dart RC, Caravati EM, McGuigan MA, editors. Medical toxicology. 3rd edn. Lippincott Williams and Wilkins; Philadelphia: 2004. pp. 21–31.
-
- Krenzelok EP, Vale JA. Position statements: gut decontamination. J Toxicol Clin Toxicol. 1997;35:695–697. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
