

Real-time in vivo imaging of retinal cell apoptosis after laser exposure
- PMID: 18281610
- PMCID: PMC2596993
- DOI: 10.1167/iovs.07-1335
Real-time in vivo imaging of retinal cell apoptosis after laser exposure
Abstract
Purpose: To investigate whether the detection of apoptosing retinal cells (DARC) could detect cells undergoing apoptosis in a laser model of retinal damage.
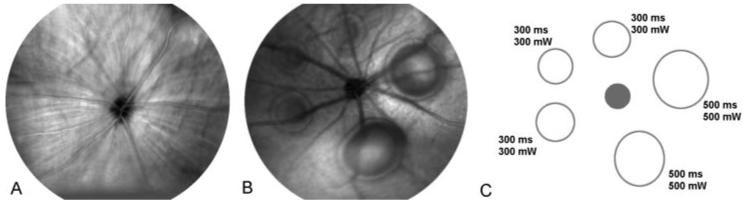
Methods: Laser lesions were placed, with the use of a frequency-doubled Nd:YAG laser, on the retina in 34 eyes of anesthetized Dark Agouti rats. Lesion size and laser-induced retinal elevation were analyzed using in vivo reflectance imaging. Development of retinal cell apoptosis was assessed using intravitreal fluorescence-labeled annexin 5 in vivo with DARC technology from baseline until 90 minutes after laser application. Histologic analysis of retinal flat mounts and cross-sections was performed.
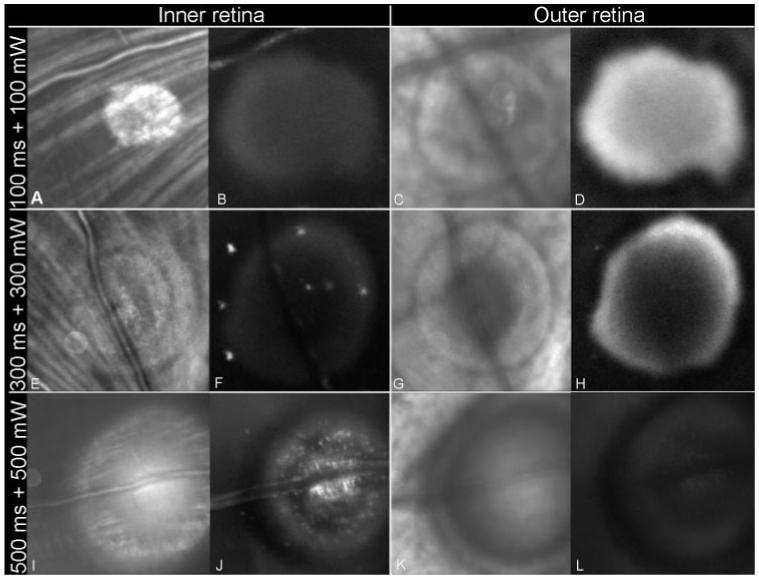
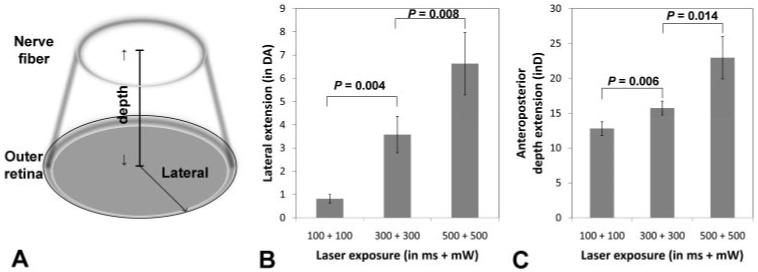
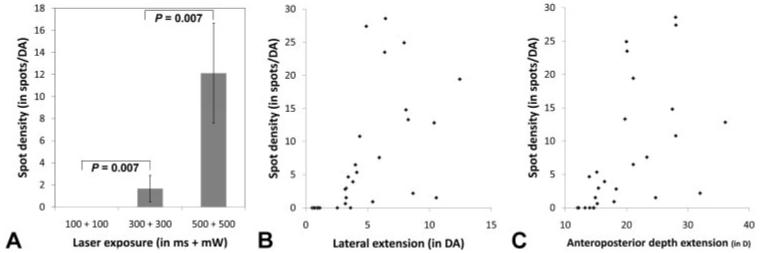
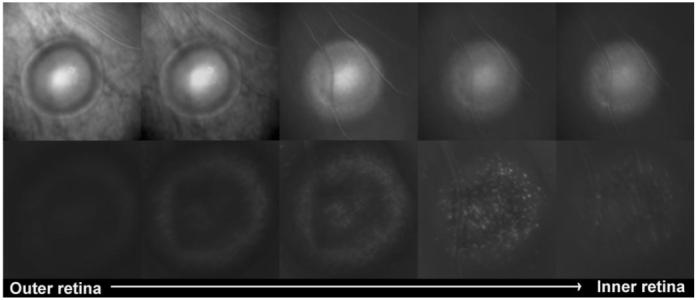
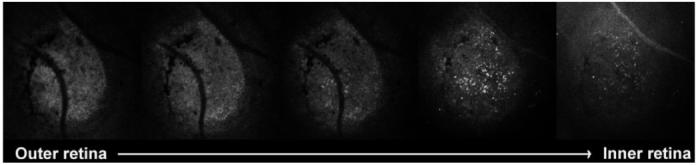
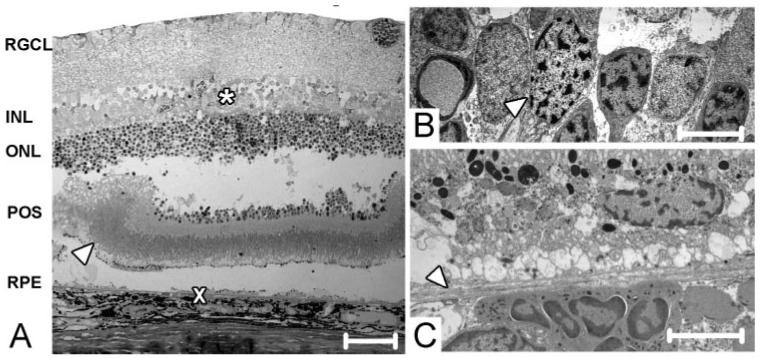
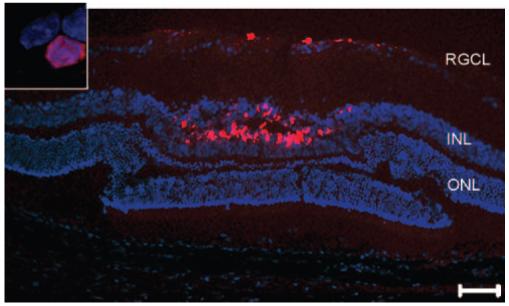
Results: The lateral and anteroposterior depth extension of the zone of laser damage was significantly larger for higher exposure settings. A strong diffuse signal, concentrated at the outer retina, was seen with DARC for low exposures (<300 ms and <300 mW). In comparison, higher exposures (>300 ms and >300 mW) resulted in detectable hyperfluorescent spots, mainly at the level of the inner retinal layers. Dose-dependent effects on spot density and positive correlation of spot density between lesion size (P < 0.0001) and retinal elevation (P < 0.0001) were demonstrated. Histology confirmed the presence of apoptosing retinal cells in the inner nuclear and the ganglion cell layers.
Conclusions: This is the first time that DARC has been used to determine apoptotic effects in the inner nuclear layer. The ability to monitor changes spatially and temporally in vivo promises to be a major advance in the real-time assessment of retinal diseases and treatment effects.
Figures
Similar articles
-
[In vivo imaging of retinal cell apoptosis following acute light exposure].Ophthalmologe. 2010 Jan;107(1):22-9. doi: 10.1007/s00347-009-1952-y. Ophthalmologe. 2010. PMID: 19499229 German.
-
Annexin-V binds subpopulation of immune cells altering its interpretation as an in vivo biomarker for apoptosis in the retina.Int J Biol Sci. 2024 Nov 11;20(15):6073-6089. doi: 10.7150/ijbs.102551. eCollection 2024. Int J Biol Sci. 2024. PMID: 39664578 Free PMC article.
-
In Vivo Detection of Retinal Ganglion Cell Stress in Rodents with DARC.Methods Mol Biol. 2023;2708:123-129. doi: 10.1007/978-1-0716-3409-7_13. Methods Mol Biol. 2023. PMID: 37558966
-
The potential of annexin-labelling for the diagnosis and follow-up of glaucoma.Cell Tissue Res. 2013 Aug;353(2):279-85. doi: 10.1007/s00441-013-1554-5. Epub 2013 Feb 1. Cell Tissue Res. 2013. PMID: 23370602 Review.
-
Annexins in Glaucoma.Int J Mol Sci. 2018 Apr 17;19(4):1218. doi: 10.3390/ijms19041218. Int J Mol Sci. 2018. PMID: 29673196 Free PMC article. Review.
Cited by
-
Imaging multiple phases of neurodegeneration: a novel approach to assessing cell death in vivo.Cell Death Dis. 2010;1(1):e3. doi: 10.1038/cddis.2009.3. Cell Death Dis. 2010. PMID: 21364622 Free PMC article.
-
Real-Time Imaging of Retinal Ganglion Cell Apoptosis.Cells. 2018 Jun 15;7(6):60. doi: 10.3390/cells7060060. Cells. 2018. PMID: 29914056 Free PMC article. Review.
-
Identification of Chlamydia pneumoniae and NLRP3 inflammasome activation in Alzheimer's disease retina.Res Sq [Preprint]. 2025 Jun 26:rs.3.rs-6658954. doi: 10.21203/rs.3.rs-6658954/v1. Res Sq. 2025. PMID: 40678205 Free PMC article. Preprint.
-
Retinal photoreceptor focal disruption secondary to accidental Nd:YAG laser exposure.Int Ophthalmol. 2011 Oct;31(5):409-12. doi: 10.1007/s10792-011-9469-1. Epub 2011 Oct 15. Int Ophthalmol. 2011. PMID: 22002418
-
Retinal safety evaluation of two-photon laser scanning in rats.Biomed Opt Express. 2019 Jun 11;10(7):3217-3231. doi: 10.1364/BOE.10.003217. eCollection 2019 Jul 1. Biomed Opt Express. 2019. PMID: 31467775 Free PMC article.
References
-
- Webb RH, Hughes GW, Delori FC. Confocal scanning laser ophthalmoscope. Appl Optics. 1987;26:1492–1499. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
