

A Prospective Study to Evaluate the Accuracy of Pulse Power Analysis to Monitor Cardiac Output in Critically Ill Patients
- PMID: 18282275
- PMCID: PMC2275227
- DOI: 10.1186/1471-2253-8-3
A Prospective Study to Evaluate the Accuracy of Pulse Power Analysis to Monitor Cardiac Output in Critically Ill Patients
Abstract
Background: Intermittent measurement of cardiac output may be performed using a lithium dilution technique (LiDCO). This can then be used to calibrate a pulse power algorithm of the arterial waveform which provides a continuous estimate of this variable. The purpose of this study was to examine the duration of accuracy of the pulse power algorithm in critically ill patients with respect to time when compared to measurements of cardiac output by an independent technique.
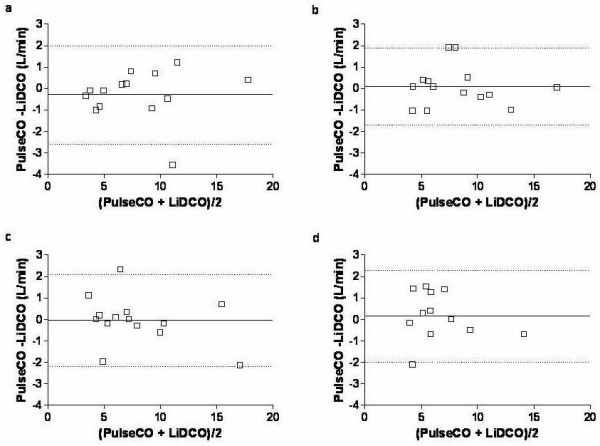
Methods: Pulse power analysis was performed on critically ill patients using a proprietary commercial monitor (PulseCO). All measurements were made using an in-dwelling radial artery line and according to manufacturers instructions. Intermittent measurements of cardiac output were made with LiDCO in order to validate the pulse power measurements. These were made at baseline and then following 1, 2, 4 and 8 hours. The LiDCO measurement was considered the reference for comparison in this study. The two methods of measuring cardiac output were then compared by linear regression and a Bland Altman analysis. An error rate for the limits of agreement (LOA) between the two techniques of less than 30% was defined as being acceptable for this study.
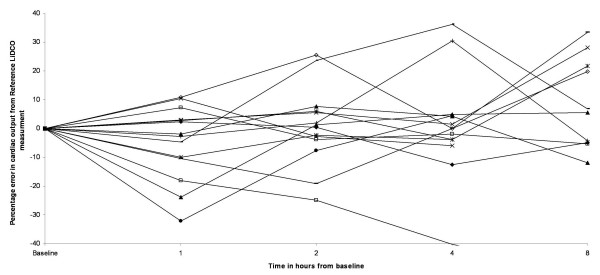
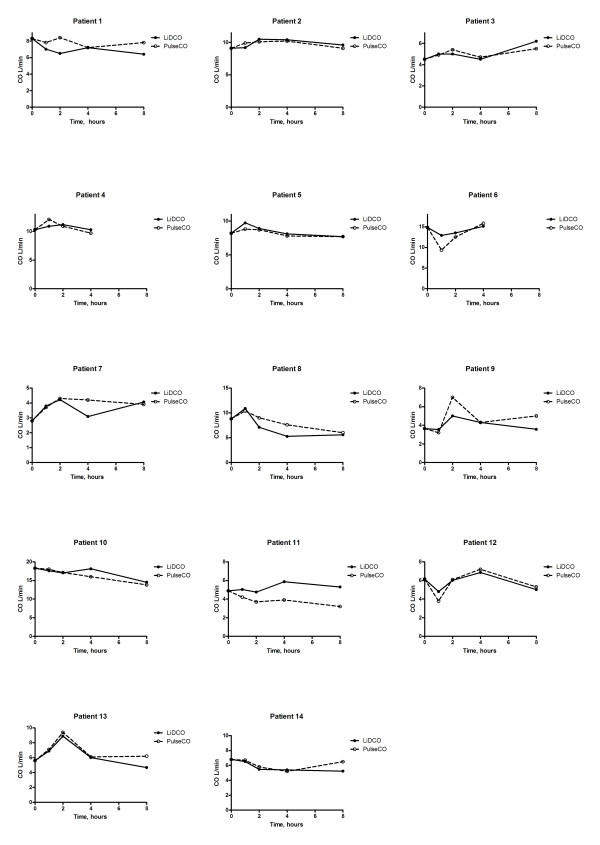
Results: 14 critically ill medical and surgical patients were enrolled over a three month period. At baseline patients showed a wide range of cardiac output (median 7.5 L/min, IQR 5.1 -9.0 L/min). The bias and limits of agreement between the two techniques was deemed acceptable for the first four hours of the study with percentage errors being 29%, 22%, and 285 respectively. The percentage error at eight hours following calibration increased to 36%. The ability of the PulseCo to detect changes in cardiac output was assessed with a similar analysis. The PulseCO tracked the changes in cardiac output with adequate accuracy for the first four hours with percentage errors being 20%, 24% and 25%. However at eight hours the error had increased to 43%.
Conclusion: The agreement between lithium dilution cardiac output and the pulse power algorithm in the PulseCO monitor remains acceptable for up to four hours in critically ill patients.
Figures

References
-
- Della RG, Costa MG, Coccia C, Pompei L, Di MP, Vilardi V, Pietropaoli P. Cardiac output monitoring: aortic transpulmonary thermodilution and pulse contour analysis agree with standard thermodilution methods in patients undergoing lung transplantation. Can J Anaesth. 2003;50:707–711. - PubMed
-
- Rodig G, Prasser C, Keyl C, Liebold A, Hobbhahn J. Continuous cardiac output measurement: pulse contour analysis vs thermodilution technique in cardiac surgical patients. Br J Anaesth. 1999;82:525–530. - PubMed
-
- Kurita T, Morita K, Kato S, Kikura M, Horie M, Ikeda K. Comparison of the accuracy of the lithium dilution technique with the thermodilution technique for measurement of cardiac output. Br J Anaesth. 1997;79:770–775. - PubMed
-
- Godje O, Hoke K, Goetz AE, Felbinger TW, Reuter DA, Reichart B, Friedl R, Hannekum A, Pfeiffer UJ. Reliability of a new algorithm for continuous cardiac output determination by pulse-contour analysis during hemodynamic instability. Crit Care Med. 2002;30:52–58. doi: 10.1097/00003246-200201000-00008. - DOI - PubMed
-
- Goedje O, Hoeke K, Lichtwarck-Aschoff M, Faltchauser A, Lamm P, Reichart B. Continuous cardiac output by femoral arterial thermodilution calibrated pulse contour analysis: comparison with pulmonary arterial thermodilution. Crit Care Med. 1999;27:2407–2412. doi: 10.1097/00003246-199911000-00014. - DOI - PubMed
LinkOut - more resources
Full Text Sources
