

Cost-effectiveness of providing full drug coverage to increase medication adherence in post-myocardial infarction Medicare beneficiaries
- PMID: 18285564
- PMCID: PMC2722033
- DOI: 10.1161/CIRCULATIONAHA.107.735605
Cost-effectiveness of providing full drug coverage to increase medication adherence in post-myocardial infarction Medicare beneficiaries
Abstract
Background: Effective therapies for the secondary prevention of coronary heart disease-related events are significantly underused, and attempts to improve adherence have often yielded disappointing results. Elimination of patient out-of-pocket costs may be an effective strategy to enhance medication use. We sought to estimate the incremental cost-effectiveness of providing full coverage for aspirin, beta-blockers, angiotensin-converting enzyme inhibitors or angiotensin receptor blockers, and statins (combination pharmacotherapy) to individuals enrolled in the Medicare drug benefit program after acute myocardial infarction.
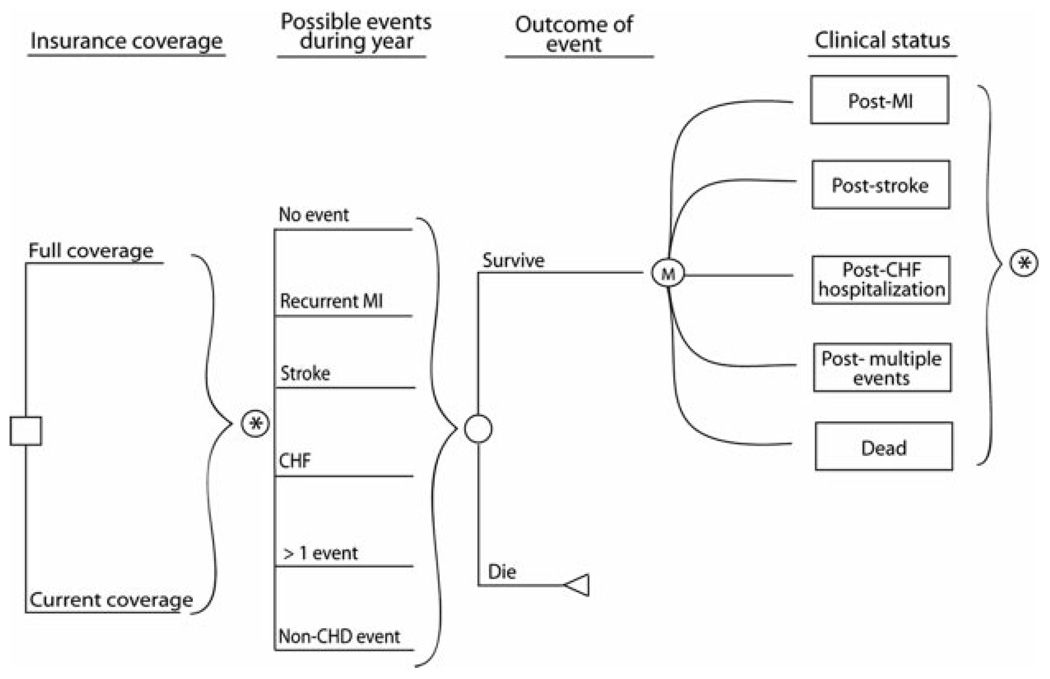
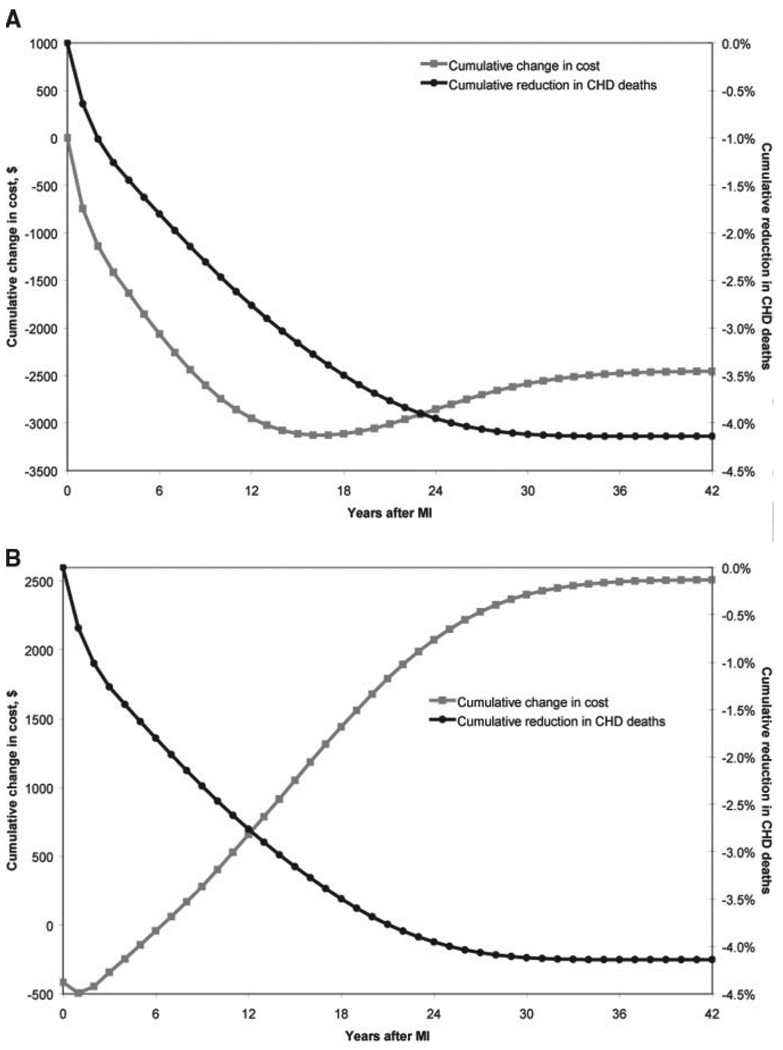
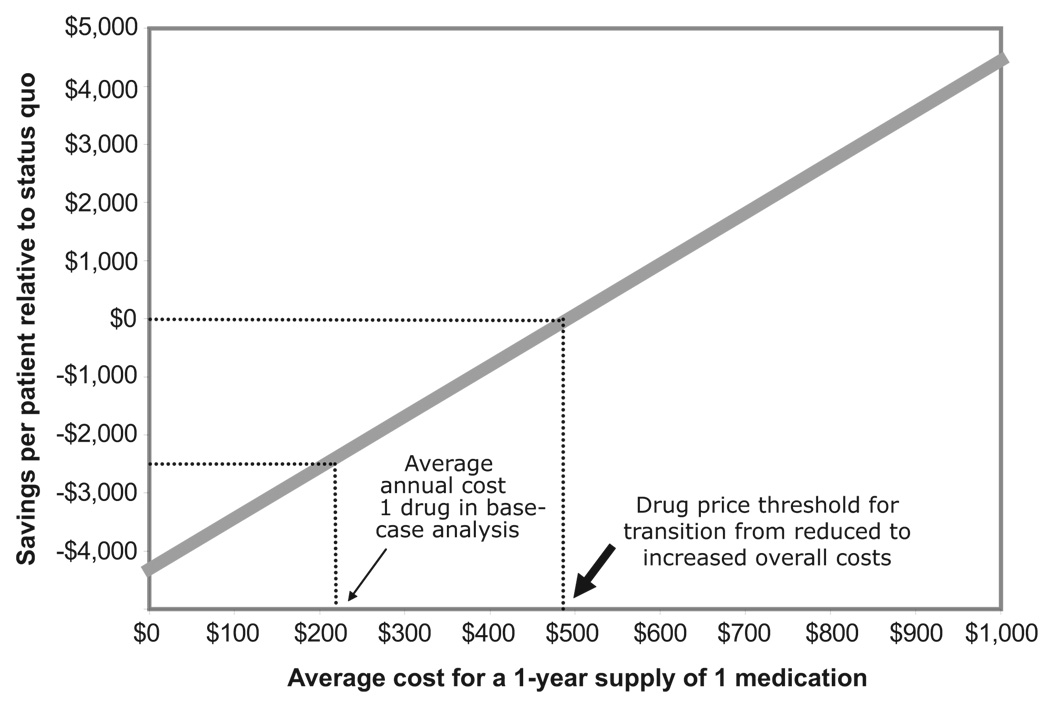
Methods and results: We created a Markov cost-effectiveness model to estimate the incremental cost-effectiveness of providing Medicare beneficiaries with full coverage for combination pharmacotherapy compared with current coverage under the Medicare Part D program. Our analysis was conducted from the societal perspective and considered a lifetime time horizon. In a sensitivity analysis, we repeated our analysis from the perspective of Medicare. In the model, post-myocardial infarction Medicare beneficiaries who received usual prescription drug coverage under the Part D program lived an average of 8.21 quality-adjusted life-years after their initial event, incurring coronary heart disease-related medical costs of $114,000. Those who received prescription drug coverage without deductibles or copayments lived an average of 8.56 quality-adjusted life-years and incurred $111,600 in coronary heart disease-related costs. Compared with current prescription drug coverage, full coverage for post-myocardial infarction secondary prevention therapies would result in greater functional life expectancy (0.35 quality-adjusted life-year) and less resource use ($2500). From the perspective of Medicare, full drug coverage was highly cost-effective ($7182/quality-adjusted life-year) but not cost saving.
Conclusions: Our analysis suggests that providing full coverage for combination therapy to post-myocardial infarction Medicare beneficiaries would save both lives and money from the societal perspective.
Figures
Comment in
-
Strategies to improve medication compliance by Medicare beneficiaries.Circulation. 2008 Mar 11;117(10):1252-4. doi: 10.1161/CIRCULATIONAHA.107.760587. Circulation. 2008. PMID: 18332276 No abstract available.
References
-
- Antman EM, Anbe DT, Armstrong PW, Bates ER, Green LA, Hand M, Hochman JS, Krumholz HM, Kushner FG, Lamas GA, Mullany CJ, Ornato JP, Pearle DL, Sloan MA, Smith SC, Jr, Alpert JS, Anderson JL, Faxon DP, Fuster V, Gibbons RJ, Gregoratos G, Halperin JL, Hiratzka LF, Hunt SA, Jacobs AK, Ornato JP. ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Revise the 1999 Guidelines for the Management of Patients With Acute Myocardial Infarction) J Am Coll Cardiol. 2004. pp. E1–E211. - PubMed
-
- McGovern PG, Jacobs DR, Jr, Shahar E, Arnett DK, Folsom AR, Blackburn H, Luepker RV. Trends in acute coronary heart disease mortality, morbidity, and medical care from 1985 through 1997: the Minnesota Heart Survey. Circulation. 2001;104:19–24. - PubMed
-
- Stafford RS, Radley DC. The underutilization of cardiac medications of proven benefit, 1990 to 2002. J Am Coll Cardiol. 2003;41:56–61. - PubMed
-
- Newby LK, LaPointe NM, Chen AY, Kramer JM, Hammill BG, DeLong ER, Muhlbaier LH, Califf RM. Long-term adherence to evidence-based secondary prevention therapies in coronary artery disease. Circulation. 2006;113:203–212. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
