

Influence of local tumor control on distant metastases and cancer related mortality after external beam radiotherapy for prostate cancer
- PMID: 18289585
- PMCID: PMC2646887
- DOI: 10.1016/j.juro.2007.11.063
Influence of local tumor control on distant metastases and cancer related mortality after external beam radiotherapy for prostate cancer
Abstract
Purpose: We report local control outcomes, as assessed by posttreatment biopsies in patients who underwent 3-dimensional conformal radiotherapy for clinically localized prostate cancer. In addition, we report the influence of local tumor control on long-term distant metastases and cause specific survival outcomes.
Materials and methods: Posttreatment prostate biopsies were performed in 339 patients who underwent 3-dimensional conformal radiotherapy for clinically localized prostate cancer. The histological outcome of prostate biopsy was classified as positive-prostatic adenocarcinoma without typical radiation induced changes or negative-no evidence of carcinoma or severe treatment effect. Median followup in this group of 339 patients was 10 years after the completion of treatment and 6.25 years after posttreatment biopsy.
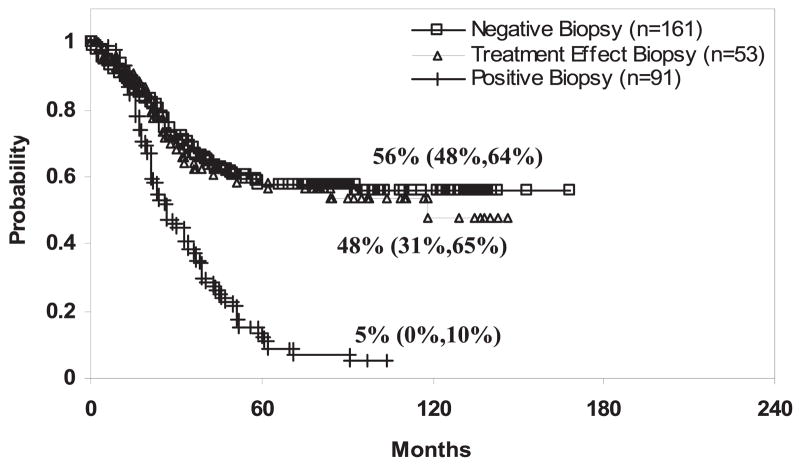
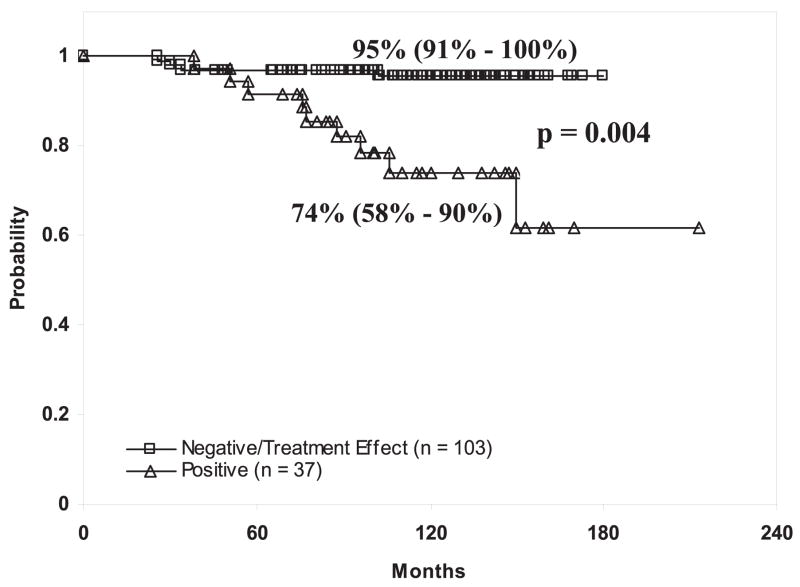
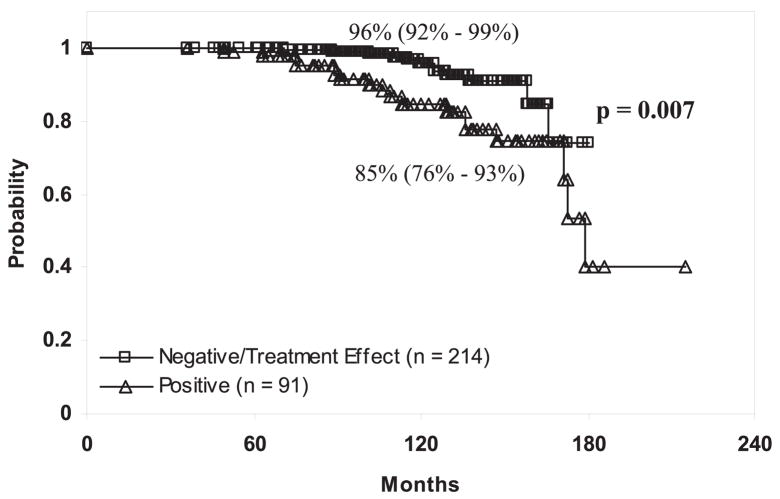
Results: Overall biopsy outcomes in these patients were positive in 32%, severe treatment effect in 21% and negative in 47%. A higher radiation dose in the intermediate and high risk subgroups was associated with a lower incidence of positive biopsy. Of patients at intermediate risk who received a dose of 75.6 or greater 24% had a positive biopsy compared to 42% who received 70.2 Gy or less (p = 0.03). In the high risk group positive treatment biopsies were noted in 51% of patients who received 70.2 Gy or less, 33% of those who received 75.6 Gy and 15% of those who received 81 Gy or greater (70.2 or less vs 75.6 Gy p = 0.07 and 75.6 vs 81 Gy or greater p = 0.05). Short course neoadjuvant androgen deprivation therapy before 3-dimensional conformal radiotherapy had a significant impact on the posttreatment biopsy outcome. Of patients who did not receive androgen deprivation therapy 42% had a positive biopsy compared to 16% who received androgen deprivation therapy (p <0.0001). Patients with negative and severe treatment effect biopsies had similar 10-year prostate specific antigen relapse-free survival outcomes that were markedly different from outcomes in those with positive treatment biopsies. Multivariate analysis indicated that the strongest predictor of biochemical failure was posttreatment biopsy status (positive vs severe treatment effect or negative p <0.001), followed by pretreatment prostate specific antigen (p = 0.05) and clinical T stage (p = 0.09). Similarly multivariate analysis revealed that a positive posttreatment biopsy was one of the strongest predictors of distant metastasis and prostate cancer death in this cohort of patients.
Conclusions: As assessed by posttreatment prostate biopsies, local control is improved with higher radiation doses. Long-term biochemical outcomes in patients with posttreatment biopsies demonstrating severe treatment effect changes were not different than those in patients with negative biopsies. We also noted that local tumor control was associated with a decrease in distant metastases and prostate cancer mortality, further highlighting the importance of achieving optimal tumor control in patients with clinically localized disease.
Figures
Comment in
-
Re: Influence of local tumor control on distant metastases and cancer related mortality after external beam radiotherapy for prostate cancer: M. J. Zelefsky, V. E. Reuter, Z. Fuks, P. Scardino and A. Shippy. J Urol 2008; 179: 1368-1373.J Urol. 2008 Nov;180(5):2258; author reply 2258. doi: 10.1016/j.juro.2008.07.074. Epub 2008 Sep 20. J Urol. 2008. PMID: 18804799 No abstract available.
References
-
- Pollack A, Zagars GK, Starkschall G, Antolak JA, Lee JJ, Huang E, et al. Prostate cancer radiation dose response: results of the M. D. Anderson phase III randomized trial. Int J Rad Oncol Biol Phys. 2002;53:1097. - PubMed
-
- Zietman AL, DeSilivio ML, Slater JD, Rossi CJ, Jr, Miller DW, Adams JA, et al. Comparison of conventional dose vs high-dose conformal radiation therapy in clinically localized adenocarcinoma of the prostate: a randomized controlled trial. JAMA. 2005;294:1233. - PubMed
-
- Peeters STH, Heembergen WD, Koper PC, van Putten WL, Slot A, Dielwart MF, et al. Dose-response in radiotherapy for localized prostate cancer: results of the Dutch multi-center randomized phase III trial comparing 68 Gy of radiotherapy with 78 Gy. J Clin Oncol. 2006;24:19190. - PubMed
-
- Dearnaley DP, Sydes MR, Graham JD, Aird EG, Bottomley D, Cowan RA, et al. Escalated-dose versus standard-dose conformal radiotherapy in prostate cancer: first results from the MRC RT01 randomised controlled trial. Lancet Oncol. 2007;8:475. - PubMed
-
- Zelefsky MJ, Fuks Z, Hunt M, Lee HJ, Lombardi D, Ling CC, et al. High dose radiation delivered by intensity modulated conformal radiotherapy improves the outcome of localized prostate cancer. J Urol. 2001;166:2321. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
