

Review
doi: 10.1016/j.smrv.2007.07.010.
Epub 2008 Mar 4.
Narcolepsy: immunological aspects
Affiliations
- PMID: 18291691
- PMCID: PMC2366136
- DOI: 10.1016/j.smrv.2007.07.010
Item in Clipboard
Review
Narcolepsy: immunological aspects
Sleep Med Rev.
2008 Apr.
Abstract
Narcolepsy with cataplexy is a debilitating sleep disorder with an estimated prevalence of about 0.05%. Narcolepsy is caused by a selective loss of hypocretin (orexin) producing neurons in the perifornical hypothalamus. Based on the very strong association with the HLA subtype DQB1*0602, it is currently hypothesized narcolepsy is caused by an autoimmune-mediated process directed at the hypocretin neurons. So far however, studies focusing on general markers of (auto)immune activation, as well as humoral immunity against the hypocretin system have not yielded consistent results supporting this hypothesis.
Figures
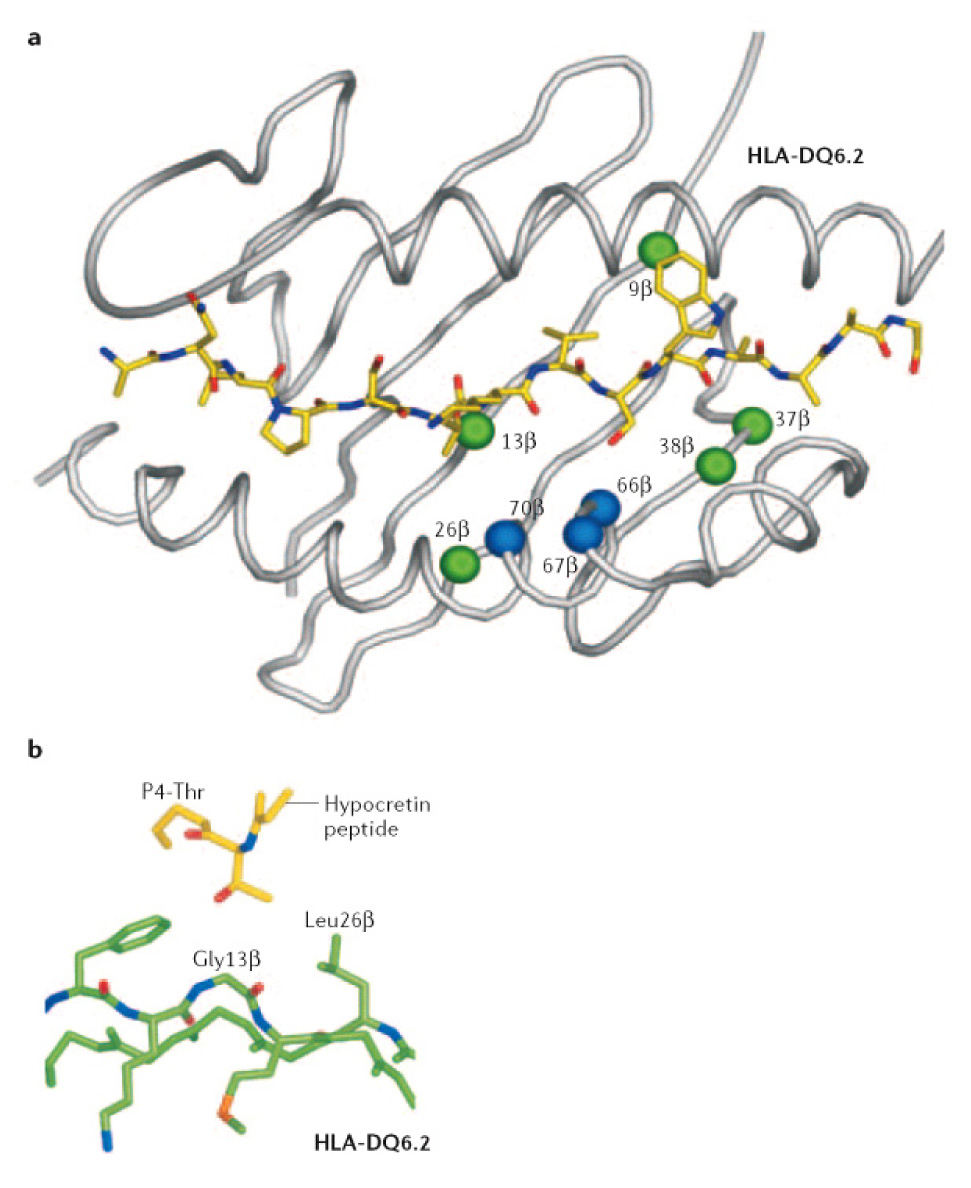
Structural representation of HLA-DQB1*0602 and 0601. A) Residues that are different between both subtypes are highlighted as spheres (green, residues contributing to peptide-binding pockets; blue, residues at the putative T-cell receptor (TCR)- recognition surface). B) Detail of the P4 binding pocket. Figure reprinted with permission from
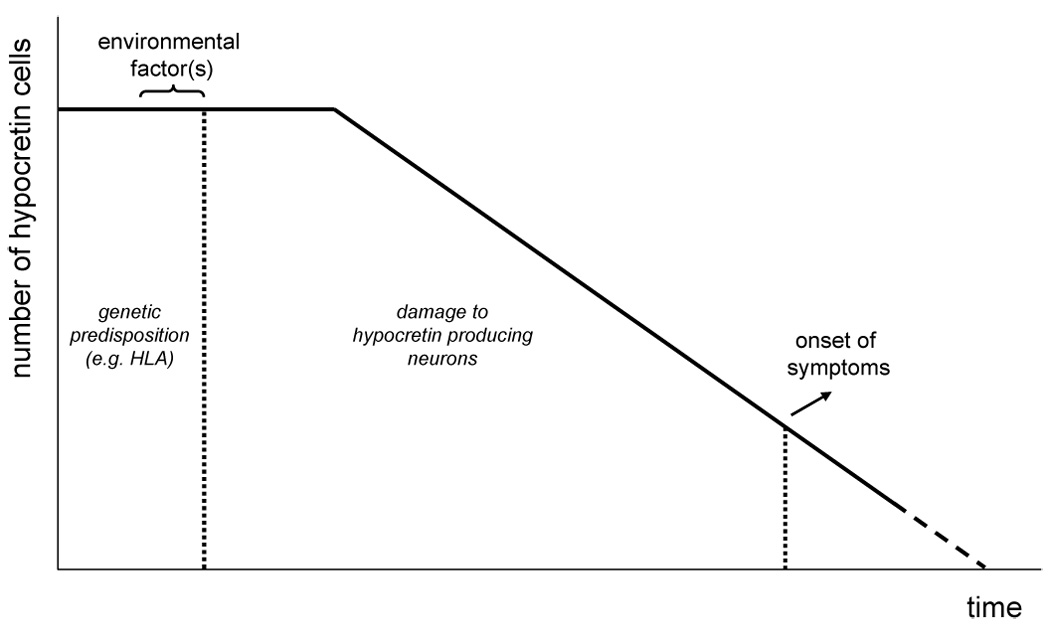
Theoretical model for the pathophysiology of narcolepsy, based on Longstreth et al. A similar model has been produced for autoimmune disorders such as type I diabetes. A specific genetic background is necessary to develop narcolepsy. Triggered by certain environmental factors, the disease process is initiated resulting in progressive damage to the hypocretin neurons. At some point, the number of remaining neurons has become so low that clinical symptoms become overt.
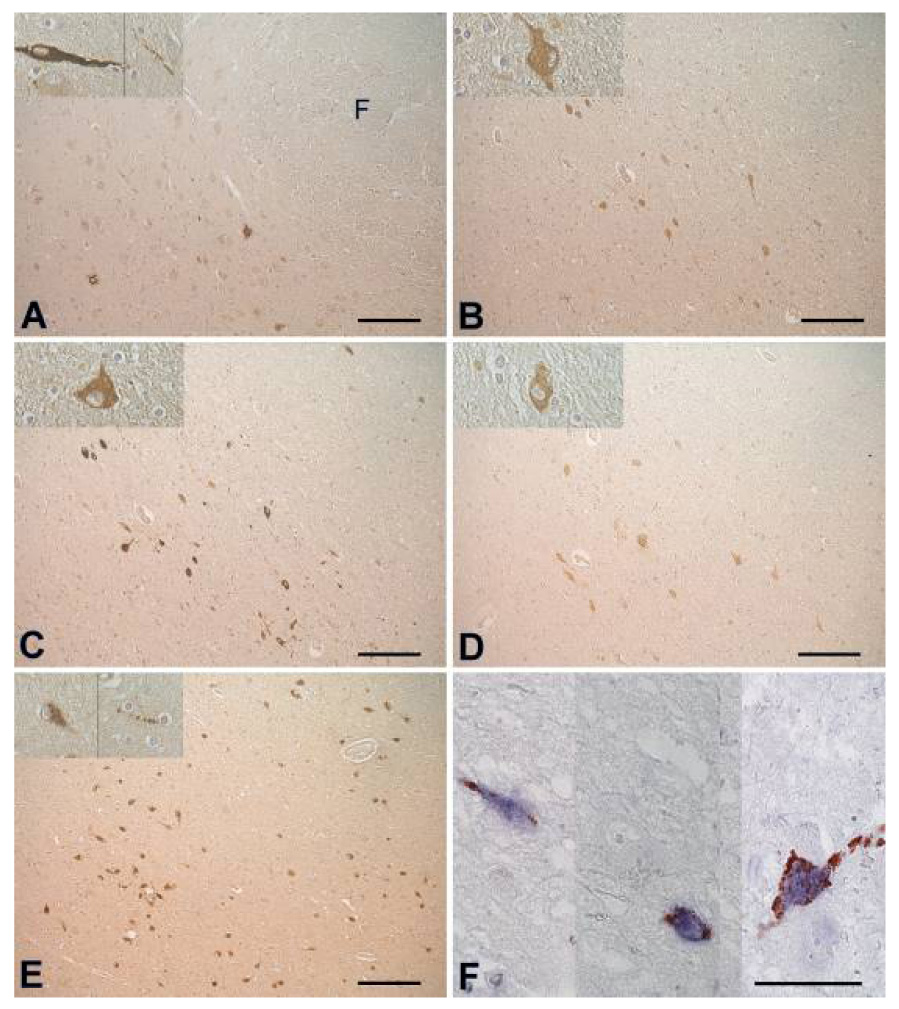
Adjacent sections from the lateral hypothalamus, stained with positive sera from 2 patients (A, B), 2 controls (C, D) and anti-hypocretin-1 (E). (F) 3 parts from sections double stained with anti-hypocretin-1 (blue) and serum of patient 1 (red). Note that no cell bodies are double stained. There are multiple bouton-like structures staining red, in close proximity of hypocretin cell bodies, suggesting nerve endings . Scale bars: (A–E): 200 µm, (F): 50 µm, (G): 1000 µm. Abbreviations: F = fornix, 3V = third ventricle. Figure reprinted with permission from
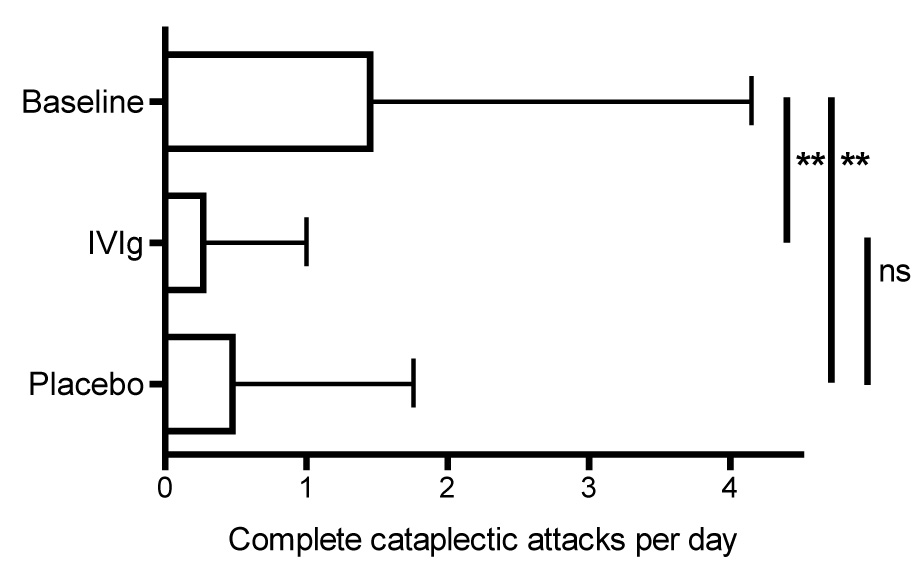
Results of a n=1 double-blind placebo-controlled study of IVIG in a patient with severe treatment refractory narcolepsy with cataplexy. Shown are the number of complete cataplexy attack per day during the baseline period, IVIG and placebo treatment. Error bars represent standard deviations. **: P < 0.001
References
-
- Overeem S, Mignot E, van Dijk JG, Lammers GJ. Narcolepsy: clinical features, new pathophysiologic insights, and future perspectives. J Clin Neurophysiol. 2001;18:78–105. - PubMed
-
- Douglas NJ. The psychosocial aspects of narcolepsy. Neurology. 1998;50:S27–S30. - PubMed
-
- Broughton WA, Broughton RJ. Psychosocial impact of narcolepsy. Sleep. 1994;17:S45–S49. - PubMed
-
- ICSD. International Classification of Sleep Disorders. Second Edition. Westchester, Il: American Academy of Sleep Medicin; 2005.
-
- Broughton R, Krupa S, Boucher B, et al. Impaired circadian waking arousal in narcolepsy-cataplexy. Sleep Res Online. 1998;1:159–165. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
