

Cost-effective osteoporosis treatment thresholds: the United States perspective
- PMID: 18292976
- PMCID: PMC2729707
- DOI: 10.1007/s00198-007-0550-6
Cost-effective osteoporosis treatment thresholds: the United States perspective
Abstract
A United States-specific cost-effectiveness analysis, which incorporated the cost and health consequences of clinical fractures of the hip, spine, forearm, shoulder, rib, pelvis and lower leg, was undertaken to identify the 10-year hip fracture probability required for osteoporosis treatment to be cost-effective for cohorts defined by age, sex, and race/ethnicity. A 3% 10-year risk of hip fracture was generally required for osteoporosis treatment to cost less than $60,000 per QALY gained.
Introduction: Rapid growth of the elderly United States population will result in so many at risk of osteoporosis that economically efficient approaches to osteoporosis care warrant consideration.
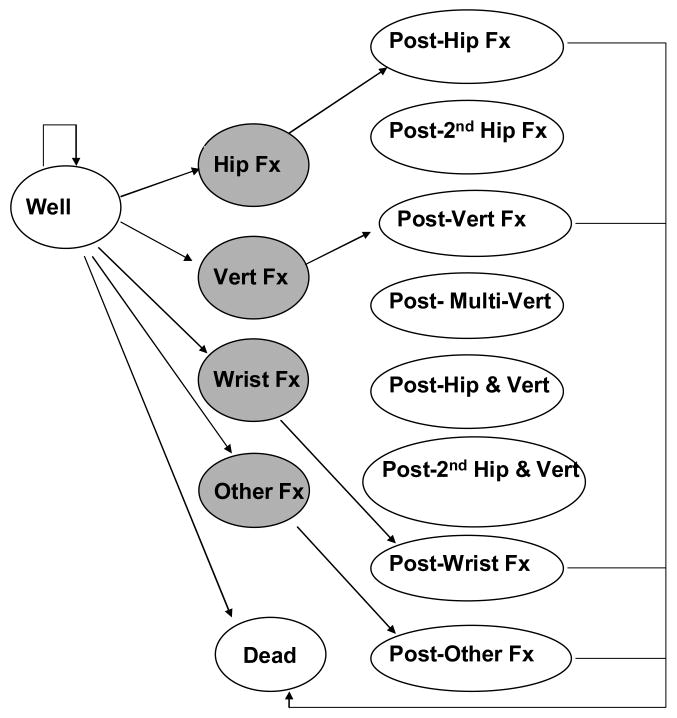
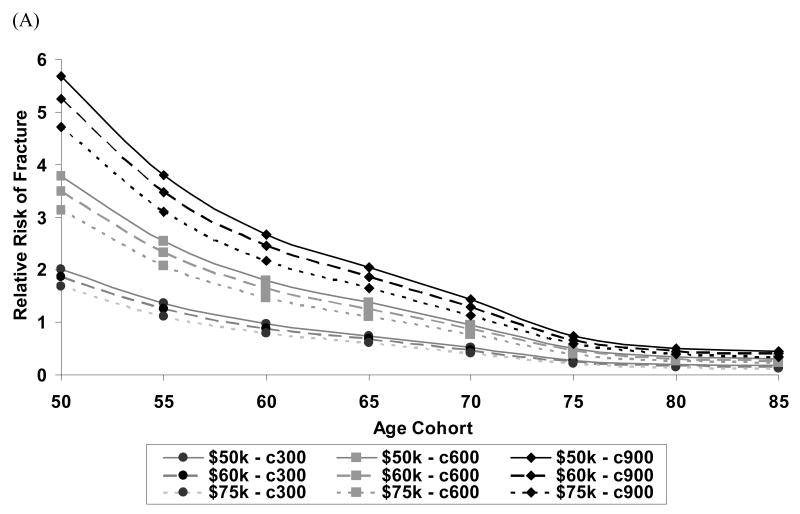
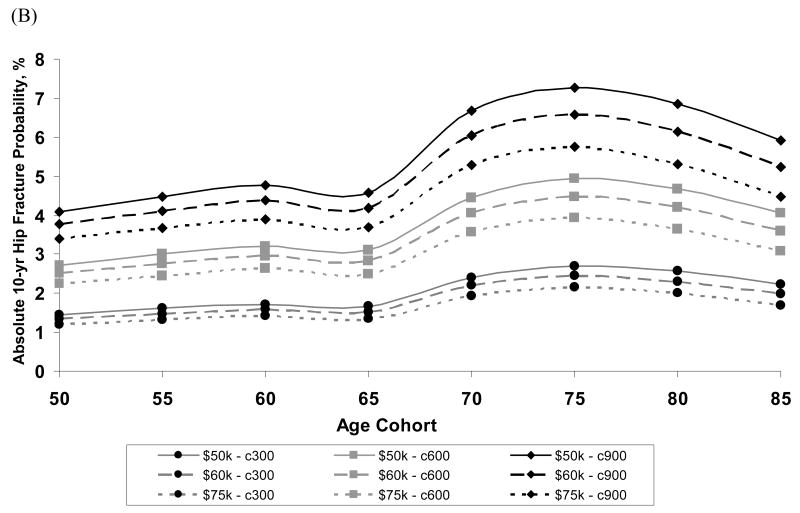
Methods: A Markov-cohort model of annual United States age-specific incidence of clinical hip, spine, forearm, shoulder, rib, pelvis and lower leg fractures, costs (2005 US dollars), and quality-adjusted life years (QALYs) was used to assess the cost-effectiveness of osteoporosis treatment ($600/yr drug cost for 5 years with 35% fracture reduction) by gender and race/ethnicity groups. To determine the 10-year hip fracture probability at which treatment became cost-effective, average annual age-specific probabilities for all fractures were multiplied by a relative risk (RR) that was systematically varied from 0 to 10 until a cost of $60,000 per QALY gained was observed for treatment relative to no intervention.
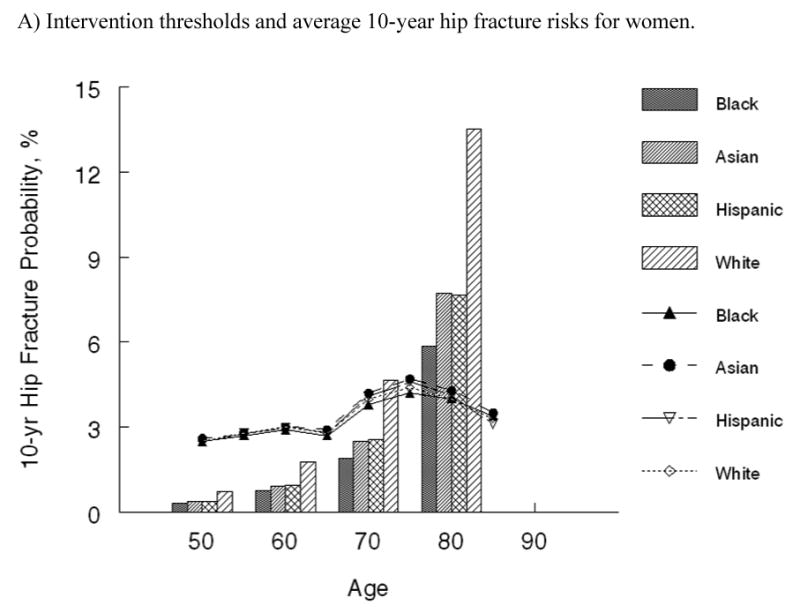
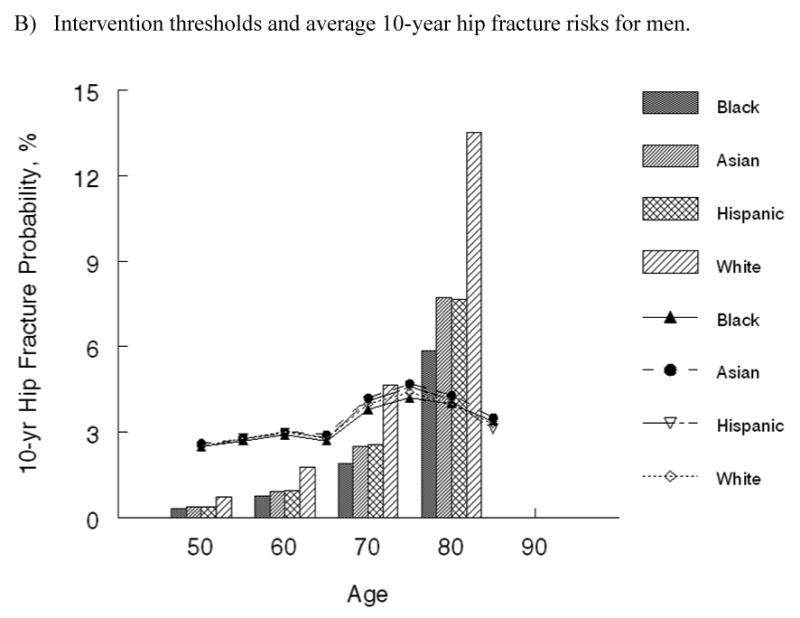
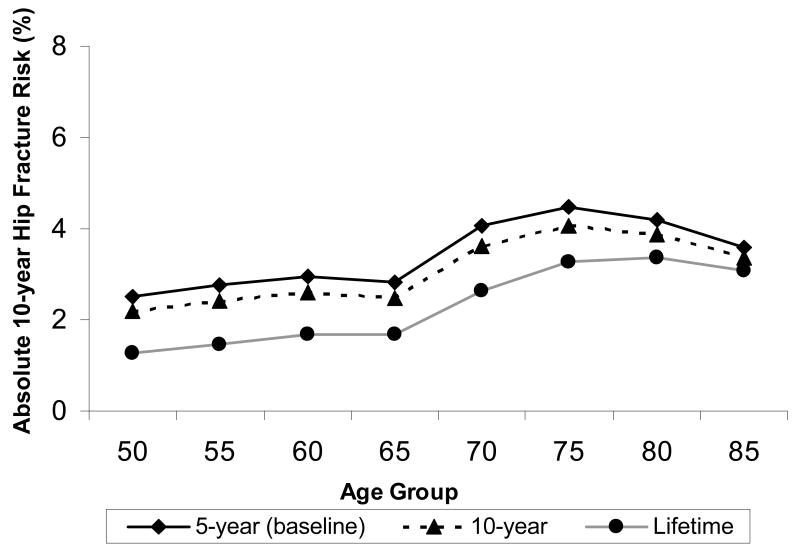
Results: Osteoporosis treatment was cost-effective when the 10-year hip fracture probability reached approximately 3%. Although the RR at which treatment became cost-effective varied markedly between genders and by race/ethnicity, the absolute 10-year hip fracture probability at which intervention became cost-effective was similar across race/ethnicity groups, but tended to be slightly higher for men than for women.
Conclusions: Application of the WHO risk prediction algorithm to identify individuals with a 3% 10-year hip fracture probability may facilitate efficient osteoporosis treatment.
Figures
References
-
- Kanis JA, Borgstrom F, De Laet C, Johansson H, Johnell O, Jonsson B, Oden A, Zethraeus N, Pfleger B, Khaltaev N. Assessment of fracture risk. Osteoporosis International. 2005;16:581–589. - PubMed
-
- Kanis JA, Black D, Cooper C, Dargent P, Dawson-Hughes B, De Laet C, Delmas P, Eisman J, Johnell O, Jonsson B, Melton L, Oden A, Papapoulos S, Pols H, Rizzoli R, Silman A, Tenenhouse A, International Osteoporosis F. National Osteoporosis F A new approach to the development of assessment guidelines for osteoporosis. Osteoporosis International. 2002;13:527–536. - PubMed
-
- Anonymous. Osteoporosis: review of the evidence for prevention, diagnosis and treatment and cost-effectiveness analysis. Introduction. Osteoporosis International. 1998;8 4:S7–80. - PubMed
-
- Department of Health and Human Services. Bone Health and Osteoporosis A Report of the Surgeon General. Rockville, MD: 2004.
-
- Burge R, Dawson-Hughes B, Solomon DH, Wong JB, King A, Tosteson A. Incidence and economic burden of osteoporosis-related fractures in the United States, 2005-2025. J Bone Miner Res. 2007;22:465–475. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
