

FRAX and the assessment of fracture probability in men and women from the UK
- PMID: 18292978
- PMCID: PMC2267485
- DOI: 10.1007/s00198-007-0543-5
FRAX and the assessment of fracture probability in men and women from the UK
Abstract
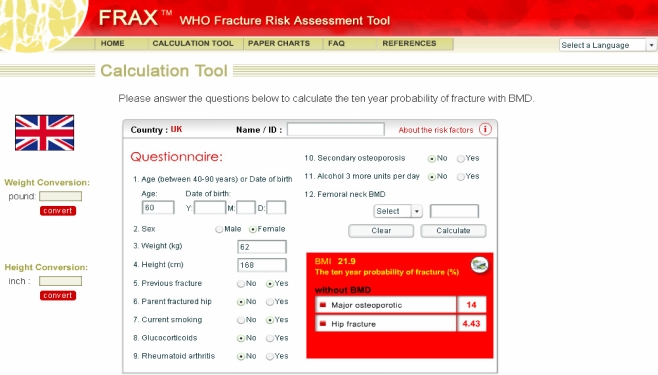
A fracture risk assessment tool (FRAX) is developed based on the use of clinical risk factors with or without bone mineral density tests applied to the UK.
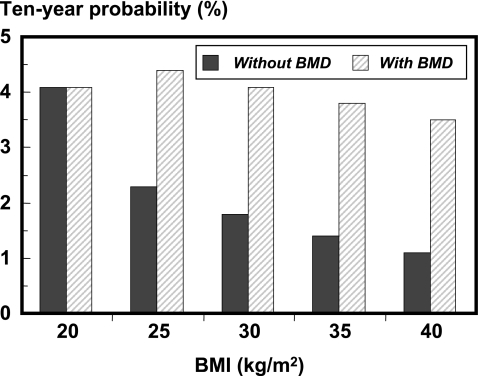
Introduction: The aim of this study was to apply an assessment tool for the prediction of fracture in men and women with the use of clinical risk factors (CRFs) for fracture with and without the use of femoral neck bone mineral density (BMD). The clinical risk factors, identified from previous meta-analyses, comprised body mass index (BMI, as a continuous variable), a prior history of fracture, a parental history of hip fracture, use of oral glucocorticoids, rheumatoid arthritis and other secondary causes of osteoporosis, current smoking, and alcohol intake 3 or more units daily.
Methods: Four models were constructed to compute fracture probabilities based on the epidemiology of fracture in the UK. The models comprised the ten-year probability of hip fracture, with and without femoral neck BMD, and the ten-year probability of a major osteoporotic fracture, with and without BMD. For each model fracture and death hazards were computed as continuous functions.
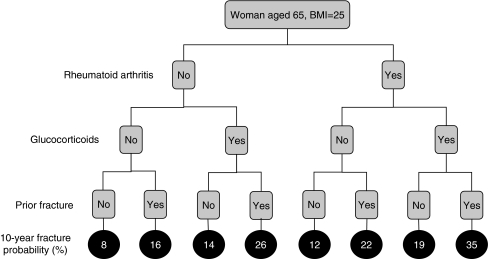
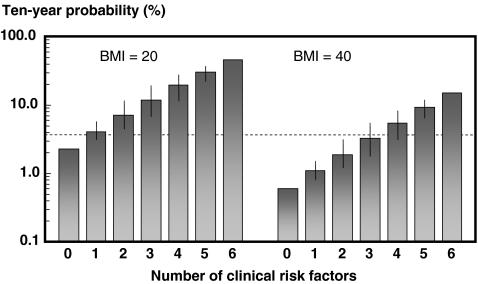
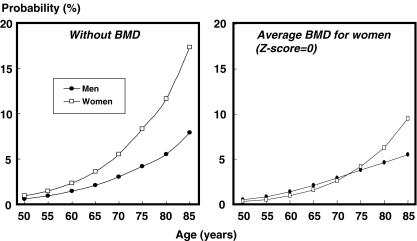
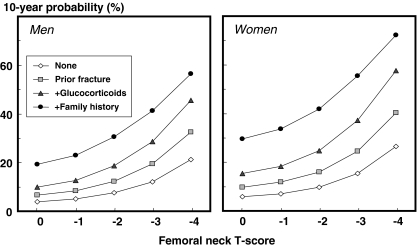
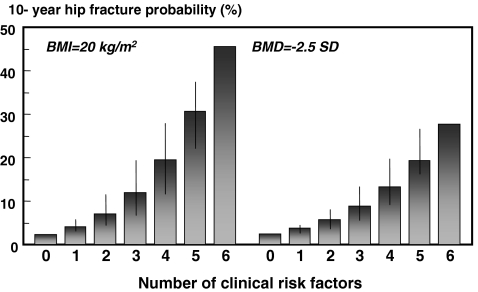
Results: Each clinical risk factor contributed to fracture probability. In the absence of BMD, hip fracture probability in women with a fixed BMI (25 kg/m(2)) ranged from 0.2% at the age of 50 years for women without CRF's to 22% at the age of 80 years with a parental history of hip fracture (approximately 100-fold range). In men, the probabilities were lower, as was the range (0.1 to 11% in the examples above). For a major osteoporotic fracture the probabilities ranged from 3.5% to 31% in women, and from 2.8% to 15% in men in the example above. The presence of one or more risk factors increased probabilities in an incremental manner. The differences in probabilities between men and women were comparable at any given T-score and age, except in the elderly where probabilities were higher in women than in men due to the higher mortality of the latter.
Conclusion: The models provide a framework which enhances the assessment of fracture risk in both men and women by the integration of clinical risk factors alone and/or in combination with BMD.
Figures
References
-
- World Health Organization (1994) Assessment of fracture risk and its application to screening for postmenopausal osteoporosis. WHO Technical Report Series 843. WHO, Geneva - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
