

Nutrition aspects in children receiving maintenance hemodialysis: impact on outcome
- PMID: 18293013
- PMCID: PMC2772959
- DOI: 10.1007/s00467-007-0728-3
Nutrition aspects in children receiving maintenance hemodialysis: impact on outcome
Abstract
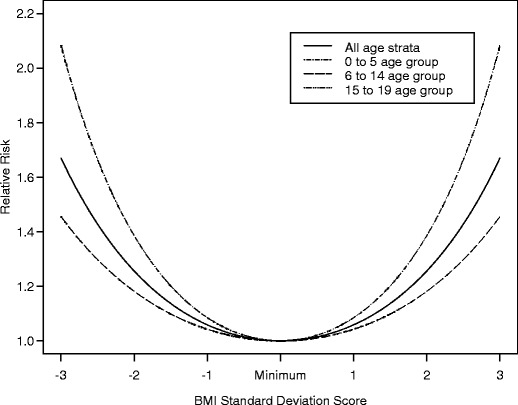
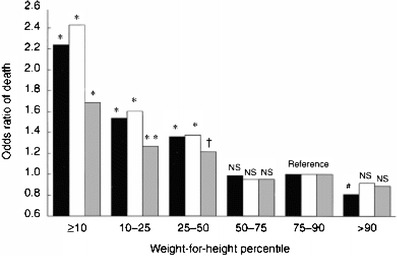
Children with end-stage renal disease (ESRD) have rates of mortality estimated to be 30-times higher than expected for age compared with those of healthy children. Physical manifestations of under-nutrition, such as body mass index (BMI) and low height standard deviation score (SDS), have been associated with increased risk of mortality. Traditional measures, such as height, weight and serum albumin concentration, may not be accurate indicators to assess the nutritional status of children receiving maintenance hemodialysis. Normalized protein catabolic rate (nPCR) has emerged as a better marker of nutritional status of such children. Meeting the special nutritional needs of these children often requires nutritional supplementation, by either the enteral or the parenteral route. Recently, in children receiving maintenance hemodialysis who are malnourished, intradialytic parenteral nutrition (IDPN) has been utilized as a means to provide additional protein and calories. This article is a state-of-the-art review of malnutrition in children receiving maintenance hemodialysis, with special focus on outcome, nPCR and IDPN.
Figures
References
-
- WHO (2001) WHO, water sanitation and health (WSH). https://doi.org/www.who.int/water_sanitation_health/diseases/malnutritio...
-
- Ahuja TS, Mitch WE. The evidence against malnutrition as a prominent problem for chronic dialysis patients. Semin Dial. 2004;17:427–431. - PubMed
-
- Kopple JD. Pathophysiology of protein-energy wasting in chronic renal failure. J Nutr. 1999;129(1S Suppl):247S–251S. - PubMed
-
- Mitch WE. Proteolytic mechanisms, not malnutrition, cause loss of muscle mass in kidney failure. J Ren Nutr. 2006;16:208–211. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
