

Unruptured large and giant carotid artery aneurysms presenting with cranial nerve palsy: comparison of clinical recovery after selective aneurysm coiling and therapeutic carotid artery occlusion
- PMID: 18296545
- PMCID: PMC8128556
- DOI: 10.3174/ajnr.A1023
Unruptured large and giant carotid artery aneurysms presenting with cranial nerve palsy: comparison of clinical recovery after selective aneurysm coiling and therapeutic carotid artery occlusion
Abstract
Background and purpose: Internal carotid artery (ICA) aneurysms may present with cranial nerve dysfunction. Therapeutic ICA occlusion, when tolerated, is an effective treatment resulting in improvement or cure of symptoms in most patients. When ICA occlusion is not tolerated, selective endovascular aneurysm occlusion can be considered. We compare recovery of cranial nerve dysfunction in patients treated with selective coil occlusion and with therapeutic ICA occlusion.
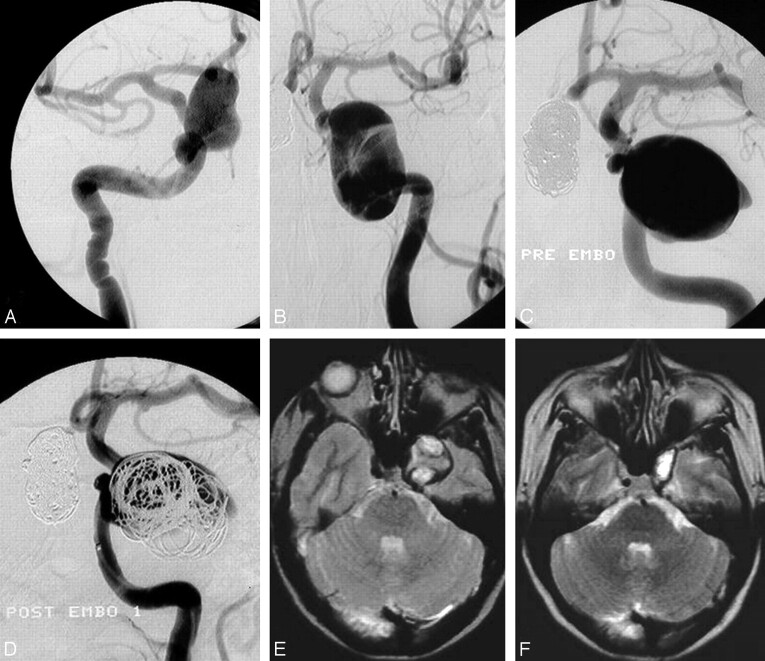
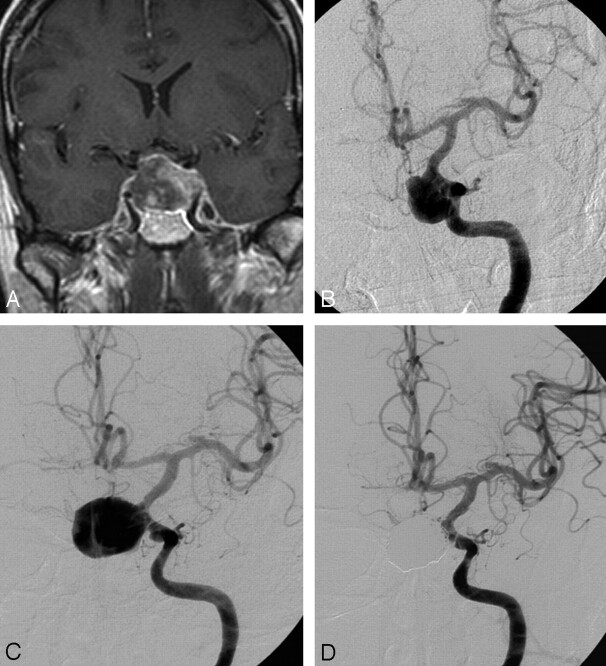
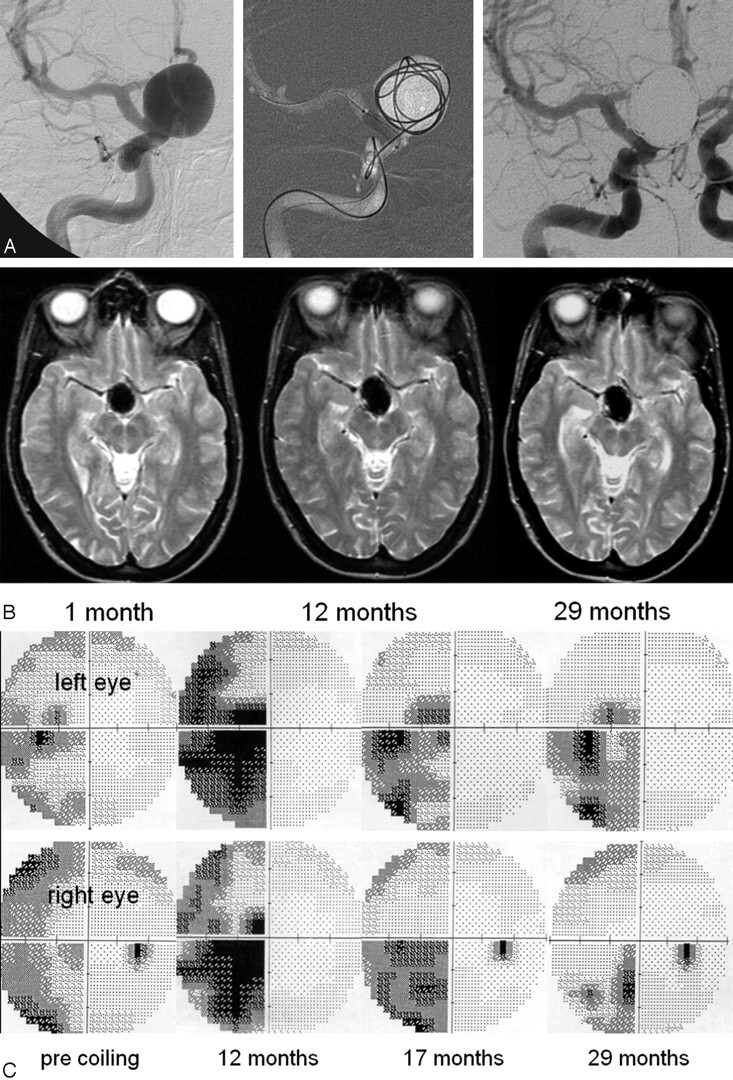
Materials and methods: In 16 patients with 17 large or giant (11-45 mm) unruptured ICA aneurysms presenting with dysfunction of cranial nerves (CN) II, III, IV, or VI, selective coil occlusion was performed. From a cohort of 39 patients with ICA aneurysms treated with ICA occlusion and long-term follow-up, we selected 31 patients with aneurysms presenting with cranial nerve dysfunction. Clinical recovery at follow-up from oculomotor dysfunction and visual symptoms was compared for both treatment modalities.
Results: Of 17 aneurysms treated with selective coiling, symptoms of cranial nerve dysfunction resolved in 3, improved in 10, and remained unchanged in 4. In 9 of 17 patients, additional coiling during follow-up was required. Of 31 aneurysms treated with carotid artery occlusion, cranial nerve dysfunction resolved in 19, improved in 9, and remained unchanged in 3. These differences were not significant. There were no complications of treatment.
Conclusion: Recovery of ICA aneurysm-induced cranial nerve dysfunction occurs in most patients, both after ICA occlusion and after selective coiling. In patients who cannot tolerate ICA occlusion, selective aneurysmal occlusion with coils is a valuable alternative.
Figures
References
-
- van der Schaaf IC, Brilstra EH, Buskens E, et al. Endovascular treatment of aneurysms in the cavernous sinus: a systematic review on balloon occlusion of the parent vessel and embolization with coils. Stroke 2002;33:313–18 - PubMed
-
- Larson JJ, Tew JM Jr., Tomsick TA, et al. Treatment of aneurysms of the internal carotid artery by intravascular balloon occlusion: long-term follow-up of 58 patients. Neurosurgery 1990;36:23–30 - PubMed
-
- de Gast AN, Sprengers ME, van Rooij WJ, et al. Midterm clinical and magnetic resonance imaging follow-up of large and giant carotid artery aneurysms after therapeutic carotid artery occlusion. Neurosurgery 2007;60:1025–29 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous