

Pathogenesis of cerebral white matter injury of prematurity
- PMID: 18296574
- PMCID: PMC2569152
- DOI: 10.1136/adc.2006.108837
Pathogenesis of cerebral white matter injury of prematurity
Abstract
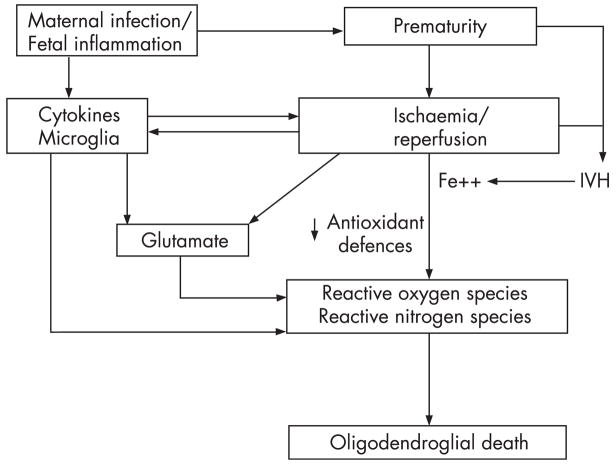
Cerebral white matter injury, characterised by loss of premyelinating oligodendrocytes (pre-OLs), is the most common form of injury to the preterm brain and is associated with a high risk of neurodevelopmental impairment. The unique cerebrovascular anatomy and physiology of the premature baby underlies the exquisite sensitivity of white matter to the abnormal milieu of preterm extrauterine life, in particular ischaemia and inflammation. These two upstream mechanisms can coexist and amplify their effects, leading to activation of two principal downstream mechanisms: excitotoxicity and free radical attack. Upstream mechanisms trigger generation of reactive oxygen and nitrogen species. The pre-OL is intrinsically vulnerable to free radical attack due to immaturity of antioxidant enzyme systems and iron accumulation. Ischaemia and inflammation trigger glutamate receptor-mediated injury leading to maturation-dependent cell death and loss of cellular processes. This review looks at recent evidence for pathogenetic mechanisms in white matter injury with emphasis on targets for prevention and treatment of injury.
Figures


References
-
- Hamilton BE, Minina AM, Martin JA, et al. Annual summary of vital statistics: 2005. Pediatrics. 2007;119:345–60. - PubMed
-
- Volpe JJ. Cerebral white matter injury of the premature infant—more common than you think. Pediatrics. 2003;112:176–9. - PubMed
-
- Dyet LE, Kennea N, Counsell SJ, et al. Natural history of brain lesions in extremely preterm infants studied with serial magnetic resonance imaging from birth and neurodevelopmental assessment. Pediatrics. 2006;118:536–48. - PubMed
-
- Hack M, Taylor HG, Drotar D, et al. Poor predictive validity of the Bayley Scales of Infant Development for cognitive function of extremely low birth weight children at school age. Pediatrics. 2005;116:333–41. - PubMed
-
- Wilson-Costello D, Friedman H, Minich N, et al. Improved neurodevelopmental outcomes for extremely low birth weight infants in 2000–2002. Pediatrics. 2007;119:37–45. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical