

Effects of statins in patients with chronic kidney disease: meta-analysis and meta-regression of randomised controlled trials
- PMID: 18299289
- PMCID: PMC2270960
- DOI: 10.1136/bmj.39472.580984.AE
Effects of statins in patients with chronic kidney disease: meta-analysis and meta-regression of randomised controlled trials
Erratum in
- BMJ. 2009;339:b2951
Abstract
Objective: To analyse the benefits and harms of statins in patients with chronic kidney disease (pre-dialysis, dialysis, and transplant populations).
Design: Meta-analysis.
Data sources: Cochrane Central Register of Controlled Trials, Medline, Embase, and Renal Health Library (July 2006).
Study selection: Randomised and quasi-randomised controlled trials of statins compared with placebo or other statins in chronic kidney disease.
Data extraction and analysis: Two reviewers independently assessed trials for inclusion, extracted data, and assessed trial quality. Differences were resolved by consensus. Treatment effects were summarised as relative risks or weighted mean differences with 95% confidence intervals by using a random effects model.
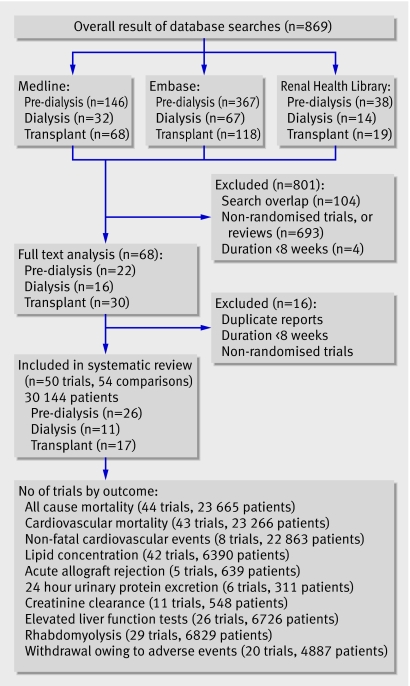
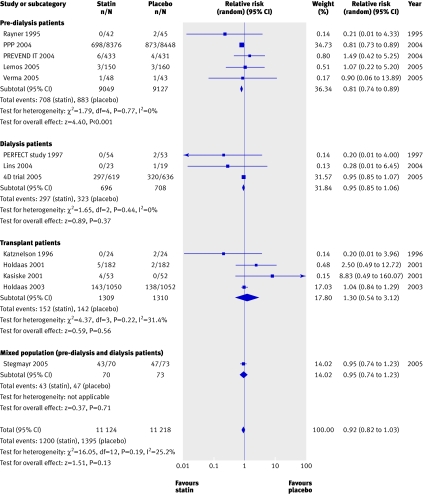
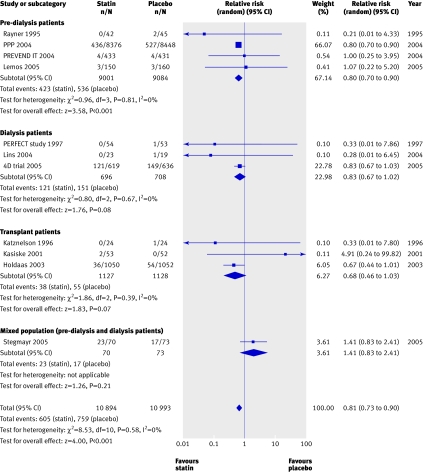
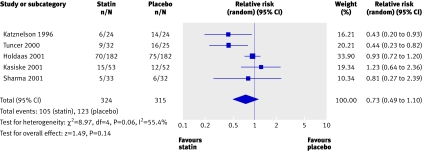
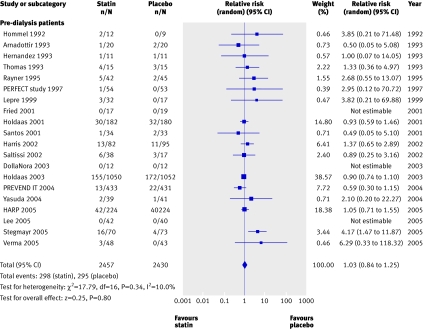
Results: Fifty trials (30 144 patients) were included. Compared with placebo, statins significantly reduced total cholesterol (42 studies, 6390 patients; weighted mean difference -42.28 mg/dl (1.10 mmol/l), 95% confidence interval -47.25 to -37.32), low density lipoprotein cholesterol (39 studies, 6216 patients; -43.12 mg/dl (1.12 mmol/l), -47.85 to -38.40), and proteinuria (g/24 hours) (6 trials, 311 patients; -0.73 g/24 hour, -0.95 to -0.52) but did not improve glomerular filtration rate (11 studies, 548 patients; 1.48 ml/min (0.02 ml/s), -2.32 to 5.28). Fatal cardiovascular events (43 studies, 23 266 patients; relative risk 0.81, 0.73 to 0.90) and non-fatal cardiovascular events (8 studies, 22 863 patients; 0.78, 0.73 to 0.84) were reduced with statins, but statins had no significant effect on all cause mortality (44 studies, 23 665 patients; 0.92, 0.82 to 1.03). Meta-regression analysis showed that treatment effects did not vary significantly with stage of chronic kidney disease. The side effect profile of statins was similar to that of placebo. Most of the available studies were small and of suboptimal quality; mortality data were provided by a few large trials only.
Conclusion: Statins significantly reduce lipid concentrations and cardiovascular end points in patients with chronic kidney disease, irrespective of stage of disease, but no benefit on all cause mortality or the role of statins in primary prevention has been established. Reno-protective effects of statins are uncertain because of relatively sparse data and possible outcomes reporting bias.
Conflict of interest statement
Competing interests: None declared.
Figures

Comment in
-
Statins for people with kidney disease.BMJ. 2008 Mar 22;336(7645):624-5. doi: 10.1136/bmj.39483.665139.80. Epub 2008 Feb 25. BMJ. 2008. PMID: 18299288 Free PMC article.
-
Assessing the benefits and harms of statin treatment in patients with chronic kidney disease.Nat Clin Pract Nephrol. 2008 Sep;4(9):470-1. doi: 10.1038/ncpneph0892. Epub 2008 Jul 15. Nat Clin Pract Nephrol. 2008. PMID: 18628740
References
-
- Coresh J, Selvin E, Stevens LA, Manzi J, Kusek JW, Eggers P, et al. Prevalence of chronic kidney disease in the United States. JAMA 2007;298:2038-47. - PubMed
-
- Foley RN, Collins AJ. End-stage renal disease in the United States: an update from the United States renal data system. J Am Soc Nephrol 2007;18:2644-8. - PubMed
-
- Ganesh S, Stack A, Levin N. Association of elevated serum PO(4), Ca × PO(4), and parathyroid hormone with cardiac mortality risk in chronic hemodialysis patients. J Am Soc Nephrol 2001;12:2131-8. - PubMed
-
- Mallamaci F, Zoccali C, Tripei G, Fermo I, Benedetto FA, Cataliotti A, et al. Hyperhomocysteinemia predicts cardiovascular outcomes in hemodialysis patients. Kidney Int 2002;61:609-14. - PubMed
-
- Jungers P, Massy ZA, Khoa TN, Fumeron C, Labrunie M, Lacour B, et al. Incidence and risk factors of atherosclerotic cardiovascular accidents in predialysis chronic renal failure patients: a prospective study. Nephrol Dial Transplant 1997;12:2597-602. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical