

Cause-specific mortality of dialysis patients after coronary revascularization: why don't dialysis patients have better survival after coronary intervention?
- PMID: 18299298
- PMCID: PMC2727291
- DOI: 10.1093/ndt/gfn038
Cause-specific mortality of dialysis patients after coronary revascularization: why don't dialysis patients have better survival after coronary intervention?
Abstract
Introduction: The risk of death after coronary revascularization is markedly higher for dialysis patients than for the general population and the cause is inadequately explained. We analyzed cause-specific mortality of dialysis patients after coronary revascularization.
Methods: This was a retrospective analysis of dialysis patients hospitalized for first surgical coronary revascularization after renal replacement therapy initiation from 1 January 1999 to 31 December 2002. Patients were identified from the US Renal Data System database (n = 1,516,251) by the International Classification of Diseases, Ninth Edition, Clinical Modification code for coronary artery bypass (CAB) surgery (36.1x). Endpoints were deaths due to all causes, all cardiac causes, cardiac arrest or arrhythmia, myocardial infarction, infection and other causes. Cause-specific mortality information was obtained from Centers for Medicare & Medicaid Services End-Stage Renal Disease Death Notification form (CMS 2746-U3).
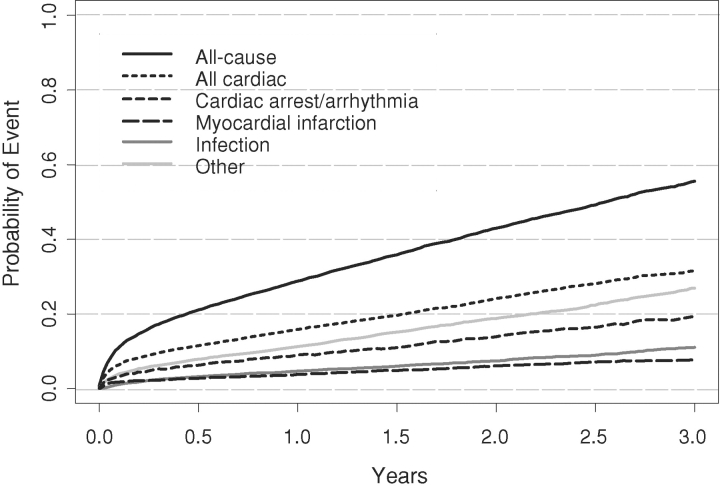
Results: For CAB patients (n = 5830), the all-cause mortality rate was 290 per 1000 patient-years and the rate for arrhythmically mediated deaths was 76 per 1000 patient-years. The largest cause of attributable mortality is cardiac arrest or arrhythmia, accounting for approximately one-fourth of all-cause mortality.
Conclusions: The risk of arrhythmically mediated death may contribute to poor long-term outcomes after coronary revascularization in dialysis patients. A treatment strategy employing coronary revascularization and other interventions to reduce the sudden cardiac death risk might improve long-term survival.
Figures
References
-
- U.S. Renal Data System. USRDS 2006 Annual Data Report. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD, 2006.
-
- Zheng ZJ, Croft JB, Giles WH, et al. Sudden cardiac death in the United States, 1989 to 1998. Circulation. 2001;104:2158–2163. - PubMed
-
- Rourke R. Role of myocardial revascularization in sudden cardiac death. Circulation. 1992;85(Suppl 1):1112–1117. - PubMed
-
- Makikallio TH, Barthel P, Schneider R, et al. Frequency of sudden cardiac death among acute myocardial infarction survivors with optimized medical and revascularization therapy. Am J Cardiol. 2006;97:480–484. - PubMed
-
- Amann K, Ritz E. Cardiac disease in chronic uremia: pathophysiology. Adv Ren Replace Ther. 1997;4:212–224. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
