

Acetabular cage survival and analysis of factors related to failure
- PMID: 18299946
- PMCID: PMC2505268
- DOI: 10.1007/s11999-008-0183-x
Acetabular cage survival and analysis of factors related to failure
Abstract
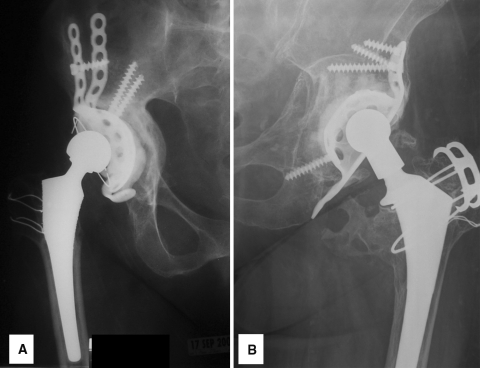
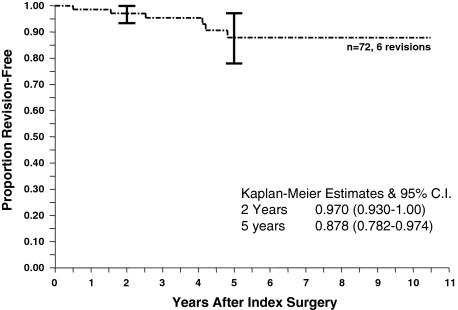
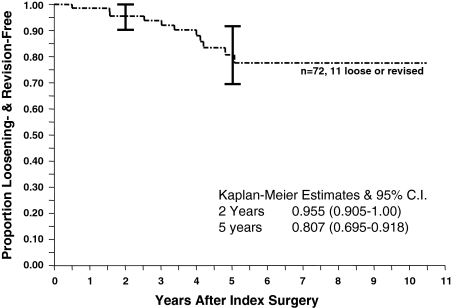
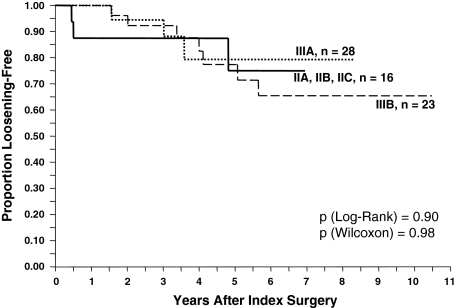
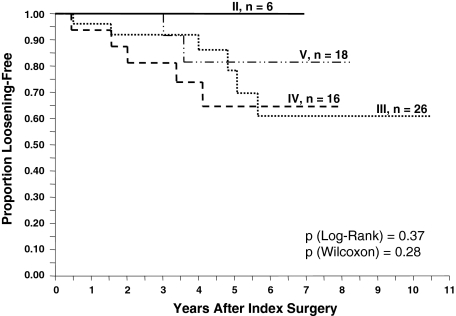
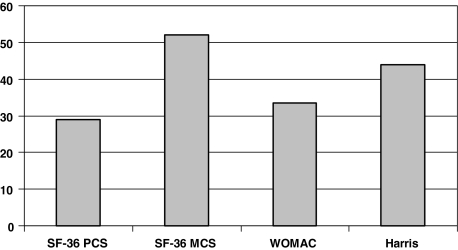
The reported results of acetabular cage reconstruction for pelvic deficiency are widely variable. Our primary question was: what is the survivorship of cage reconstruction with a primary end point of cage revision and secondary end points of radiographic loosening and any reoperation? Secondary questions were: which factors predict cage failure, and what is the functional outcome (SF-36, WOMAC, Harris hip score) of this reconstructive method? We reviewed 72 cage reconstructions in 68 patients. Minimum followup was 1.2 years (mean, 5.1 years; range, 1.2-10.7 years). Five-year cage revision-free survivorship was 87.8%. Five-year loosening-free and acetabular reoperation-free survivorships were 80.7% and 81.3%, respectively. No single preoperative factor (age, gender, severity of pelvic defect, degree of heterotopic ossification, difference in limb lengths and centers of rotation) or intraoperative factor (type of bone graft, type of cage, changes in limb length and center of rotation) predicted cage failure. Functional outcomes were 28.9 (SF-36 Physical Component), 52.4 (SF-36 Mental Component), 33.7 (WOMAC), and 44.2 (Harris). We judged these outcomes acceptable for this sometimes challenging problem. Future techniques for treating pelvic deficiency will need to be compared with these and other outcomes in the literature.
Level of evidence: Level IV, therapeutic study.
Figures

References
-
- Bellamy N, Buchanan WW, Goldsmith CH, Campbell J, Stitt LW. Validation study of WOMAC: a health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J Rheumatol. 1988;15:1833–1840. - PubMed
-
- Berry DJ, Lewallen DG, Hanssen AD, Cabanela ME. Pelvic discontinuity in revision total hip arthroplasty. J Bone Joint Surg Am. 1999;81:1692–1702. - PubMed
-
- Berry DJ, Müller ME. Revision arthroplasty using an anti-protrusio cage for massive acetabular bone deficiency. J Bone Joint Surg Br. 1992;74:711–715. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
