

Determinants of tracheostomy decannulation: an international survey
- PMID: 18302759
- PMCID: PMC2374629
- DOI: 10.1186/cc6802
Determinants of tracheostomy decannulation: an international survey
Abstract
Background: Although tracheostomy is probably the most common surgical procedure performed on critically ill patients, it is unknown when a tracheostomy tube can be safely removed.
Methods: We performed a cross-sectional survey of physicians and respiratory therapists with expertise in the management of tracheostomized patients at 118 medical centers to characterize contemporary opinions about tracheostomy decannulation practice and to define factors that influence these practices.
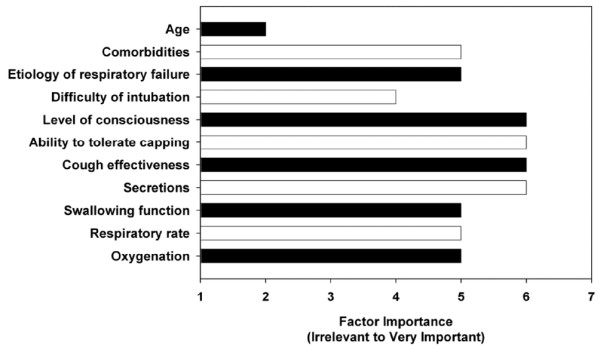
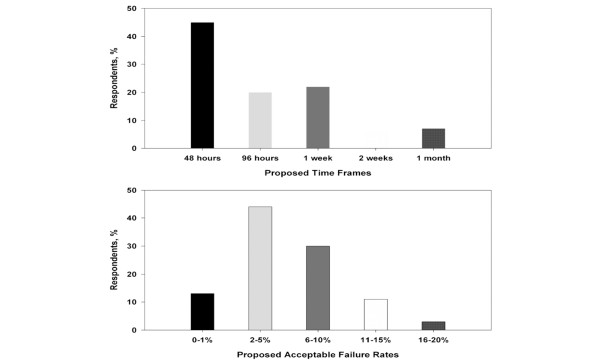
Results: We surveyed 309 clinicians, of whom 225 responded (73%). Clinicians rated patient level of consciousness, ability to tolerate tracheostomy tube capping, cough effectiveness, and secretions as the most important factors in the decision to decannulate a patient. Decannulation failure was defined as the need to reinsert an artificial airway within 48 hours (45% of respondents) to 96 hours (20% of respondents) of tracheostomy removal, and 2% to 5% was the most frequent recommendation for an acceptable recannulation rate (44% of respondents). In clinical scenarios, clinicians who worked in chronic care facilities (30%) were less likely to recommend decannulation than clinicians who worked in weaning (47%), rehabilitation (53%), or acute care (55%) facilities (p = 0.015). Patients were most likely to be recommended for decannulation if they were alert and interactive (odds ratio [OR] 4.76, 95% confidence interval [CI] 3.27 to 6.90; p < 0.001), had a strong cough (OR 3.84, 95% CI 2.66 to 5.54; p < 0.001), had scant thin secretions (OR 2.23, 95% CI 1.56 to 3.19; p < 0.001), and required minimal supplemental oxygen (OR 2.04, 95% CI 1.45 to 2.86; p < 0.001).
Conclusion: Patient level of consciousness, cough effectiveness, secretions, and oxygenation are important determinants of clinicians' tracheostomy decannulation opinions. Most surveyed clinicians defined decannulation failure as the need to reinsert an artificial airway within 48 to 96 hours of planned tracheostomy removal.
Figures
Comment in
-
Tracheostomy decannulation: marathons and finish lines.Crit Care. 2008;12(2):128. doi: 10.1186/cc6833. Epub 2008 Mar 31. Crit Care. 2008. PMID: 18394184 Free PMC article.
References
-
- Apezteguia C, Rios F, Pezzola D. Tracheostomy in patients with respiratory failure receiving mechanical ventilation: how, when, and for whom? In: Esteban A, Anzueto A, Cook DJ, editor. Evidence-Based Management of Patients with Respiratory Failure. Vol. 41. Berlin: Springer; 2004. pp. 121–134.
-
- Esteban A, Anzueto A, Alía I, Gordo F, Apezteguía C, Pálizas F, Cide D, Goldwaser R, Soto L, Bugedo G, Rodrigo C, Pimentel J, Raimondi G, Tobin MJ. How is mechanical ventilation employed in the intensive care unit? An international utilization review. Am J Respir Crit Care Med. 2000;161:1450–1458. - PubMed
-
- Frutos-Vivar F, Esteban A, Apezteguía C, Anzueto A, Nightingale P, González M, Soto L, Rodrigo C, Raad J, David CM, Matamis D, D' Empaire G, International Mechanical Ventilation Study Group Outcome of mechanically ventilated patients who require a tracheostomy. Crit Care Med. 2005;33:290–298. doi: 10.1097/01.CCM.0000150026.85210.13. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
