

Prospective assessment of lymphatic dissemination in endometrial cancer: a paradigm shift in surgical staging
- PMID: 18304622
- PMCID: PMC3667391
- DOI: 10.1016/j.ygyno.2008.01.023
Prospective assessment of lymphatic dissemination in endometrial cancer: a paradigm shift in surgical staging
Abstract
Objective: To prospectively assess pelvic and para-aortic lymph node metastases in endometrial cancer with lymphatic dissemination, emphasizing the examination of para-aortic metastases relative to the inferior mesenteric artery (IMA).
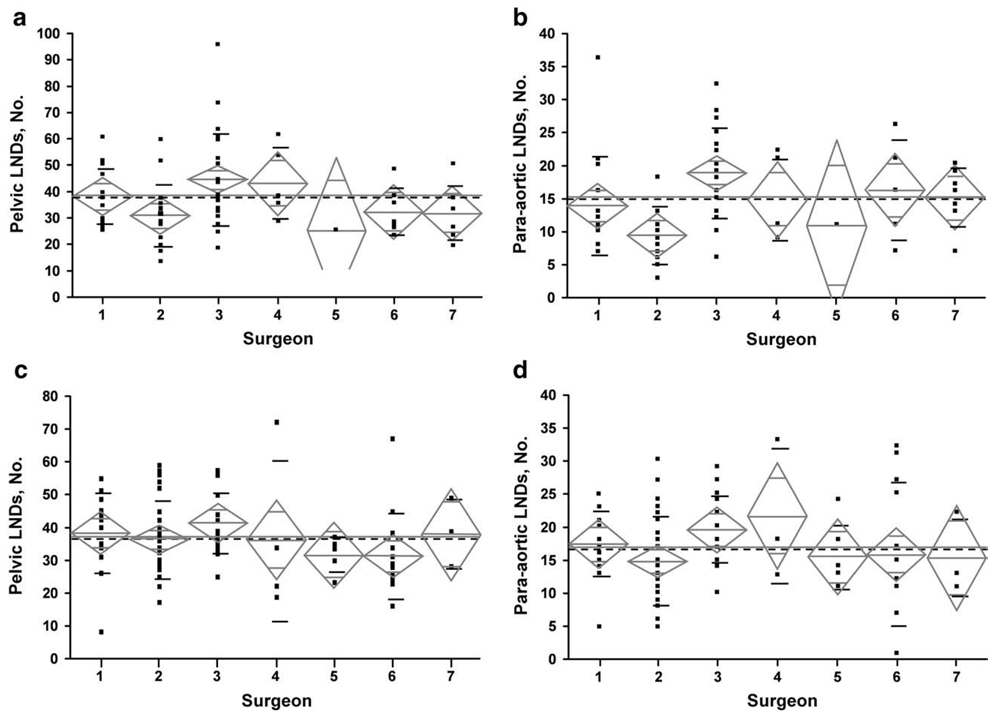
Methods: Over 36 months, 422 consecutive patients were managed by predefined surgical guidelines differentiating low-risk patients from patients at risk for dissemination requiring systematic lymphadenectomy. Low risk was defined as grade 1 or 2 endometrioid type with myometrial invasion (MI) < or = 50% and primary tumor diameter (PTD) < or = 2 cm. Pelvic and para-aortic lymph nodes were submitted separately, with nodes identified from all 8 pelvic and 4 para-aortic node-bearing basins. Surgical quality assessments examined median node counts (primary surrogate for quality) and nodes harvested above and below the IMA and excised gonadal veins (secondary surrogates).
Results: Lymphadenectomy was not required in 27% of patients (all low risk) and in 33% (n=112) of endometrioid cases. However, 22 patients (20%) of this latter cohort had lymphadenectomy and all lymph nodes were negative. Sixty-three (22%) of 281 patients undergoing lymphadenectomy had lymph node metastases: both pelvic and para-aortic in 51%, only pelvic in 33%, and isolated to the para-aortic area in 16%. Therefore, 67% of patients with lymphatic dissemination had para-aortic lymph node metastases. Furthermore, 77% of patients with para-aortic node involvement had metastases above the IMA, whereas nodes in the ipsilateral para-aortic area below the IMA and ipsilateral common iliac basin were declared negative in 60% and 71%, respectively. Gonadal veins were excised in 25 patients with para-aortic node metastases; 7 patients (28%) had documented metastatic involvement of gonadal veins or surrounding soft tissue.
Conclusions: The high rate of lymphatic metastasis above the IMA indicates the need for systematic pelvic and para-aortic lymphadenectomy (vs sampling) up to the renal vessels. The latter should include consideration of excision of the gonadal veins. Conversely, lymphadenectomy does not benefit patients with grade 1 and 2 endometrioid lesions with MI < or = 50% and PTD < or = 2 cm.
Figures

Comment in
-
Surgical management of endometrial cancer: how much is enough?Gynecol Oncol. 2008 Apr;109(1):1-3. doi: 10.1016/j.ygyno.2008.02.013. Gynecol Oncol. 2008. PMID: 18374816 No abstract available.
-
Endometrial cancer and lymph node surgery: the spins continue--a case for reason.Gynecol Oncol. 2008 Oct;111(1):3-6. doi: 10.1016/j.ygyno.2008.07.004. Epub 2008 Aug 9. Gynecol Oncol. 2008. PMID: 18692881 No abstract available.
References
-
- Creasman WT, Odicino F, Maisonneuve P, Beller U, Benedet JL, Heintz AP, et al. Carcinoma of the corpus uteri. J Epidemiol Biostat. 2001;6:47–86. - PubMed
-
- Creutzberg CL, van Putten WL, Koper PC, Lybeert ML, Jobsen JJ, Wárlám-Rodenhuis CC, et al. PORTEC (Post Operative Radiation Therapy in Endometrial Carcinoma) Study Group. Surgery and post-operative radiotherapy versus surgery alone for patients with stage-1 endometrial carcinoma: multicentre randomised trial. Lancet. 2000;355:1404–1411. - PubMed
-
- Gynecologic Oncology Group. Keys HM, Roberts JA, Brunetto VL, Zaino RJ, Spirtos NM, Bloss JD, et al. A phase III trial of surgery with or without adjunctive external pelvic radiation therapy in intermediate risk endometrial adenocarcinoma: a Gynecologic Oncology Group study. Gynecol Oncol 2004;92:744-51 Erratum in: Gynecol Oncol. 2004;94:241–242. - PubMed
-
- Nomura H, Aoki D, Suzuki N, Susumu N, Suzuki A, Tamada Y, et al. Analysis of clinicopathologic factors predicting para-aortic lymph node metastasis in endometrial cancer. Int J Gynecol Cancer. 2006;16:799–804. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
