

Prevalence of high-risk human papillomavirus types in Mexican women with cervical intraepithelial neoplasia and invasive carcinoma
- PMID: 18307798
- PMCID: PMC2294112
- DOI: 10.1186/1750-9378-3-3
Prevalence of high-risk human papillomavirus types in Mexican women with cervical intraepithelial neoplasia and invasive carcinoma
Abstract
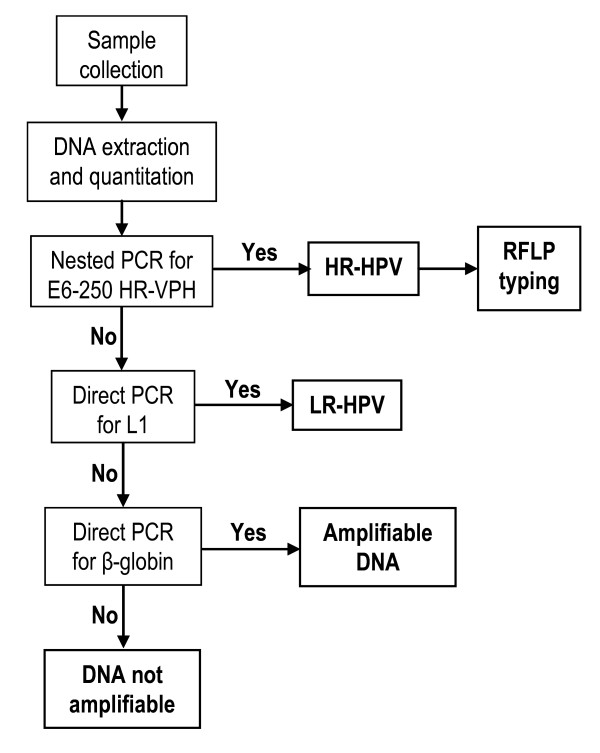
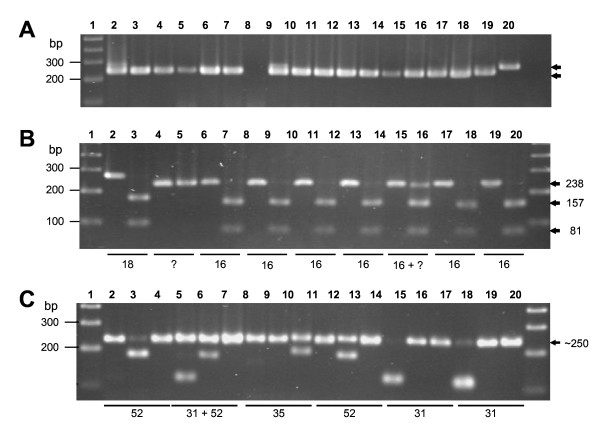
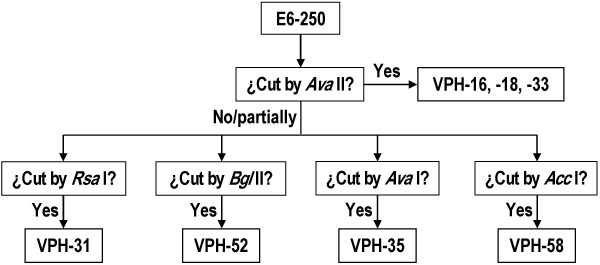
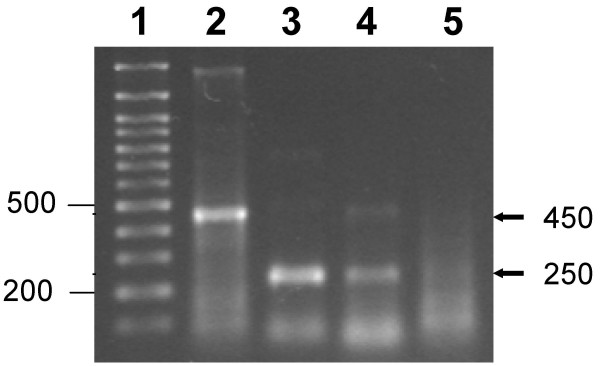
Background: Prevalence of high risk (HR) human papillomavirus (HPV) types in the states of San Luis Potosí (SLP) and Guanajuato (Gto), Mexico, was determined by restriction fragment length-polymorphism (RFLP) analysis on the E6 ~250 bp (E6-250) HR-HPV products amplified from cervical scrapings of 442 women with cervical intraepithelial neoplasia and invasive carcinoma (280 from SLP and 192 from Gto). Fresh cervical scrapings for HPV detection and typing were obtained from all of them and cytological and/or histological diagnoses were performed on 383.
Results: Low grade intraepithelial squamous lesions (LSIL) were diagnosed in 280 cases (73.1%), high grade intraepithelial squamous lesions (HSIL) in 64 cases (16.7%) and invasive carcinoma in 39 cases (10.2%). In the 437 cervical scrapings containing amplifiable DNA, only four (0.9%) were not infected by HPV, whereas 402 (92.0%) were infected HR-HPV and 31 (7.1%) by low-risk HPV. RFLP analysis of the amplifiable samples identified infections by one HR-HPV type in 71.4%, by two types in 25.9% and by three types in 2.7%. The overall prevalence of HR-HPV types was, in descending order: 16 (53.4%) > 31 (15.6%) > 18 (8.9%) > 35 (5.6) > 52 (5.4%) > 33 (1.2%) > 58 (0.7%) = unidentified types (0.7%); in double infections (type 58 absent in Gto) it was 16 (88.5%) > 31 (57.7%) > 35 (19.2%) > 18 (16.3%) = 52 (16.3%) > 33 (2.8%) = 58 (2.8%) > unidentified types (1.0%); in triple infections (types 33 and 58 absent in both states) it was 16 (100.0%) > 35 (54.5%) > 31 (45.5%) = 52 (45.5%) > 18 (27.3%). Overall frequency of cervical lesions was LSIL (73.1%) > HSIL (16.7%) > invasive cancer (10.2%). The ratio of single to multiple infections was inversely proportional to the severity of the lesions: 2.46 for LSIL, 2.37 for HSIL and 2.15 for invasive cancer. The frequency of HR-HPV types in HSIL and invasive cancer lesions was 16 (55.0%) > 31 (18.6%) > 35 (7.9%) > 52 (7.1%) > 18 (4.3%) > unidentified types (3.6%) > 33 (2.9%) > 58 (0.7%).
Conclusion: Ninety percent of the women included in this study were infected by HR-HPV, with a prevalence 1.14 higher in Gto. All seven HR-HPV types identifiable with the PCR-RFLP method used circulate in SLP and Gto, and were diagnosed in 99.3% of the cases. Seventy-one percent of HR-HPV infections were due to a single type, 25.9% were double and 2.7% were triple. Overall frequency of lesions was LSIL (73.1%) > HSIL (16.7%) > invasive cancer (10.2%), and the ratio of single to multiple infections was inversely proportional to severity of the lesions: 2.46 for LSIL, 2.37 for HSIL and 2.15 for invasive cancer. The frequency of HR-HPV types found in HSIL and invasive cancer was 16 (55.0%) > 31 (18.6%) > 35 (7.9%) > 52 (7.1%) > 18 (4.3%) > unidentified types (3.6%) > 33 (2.9%) > 58 (0.7%). Since the three predominant types (16, 31 and 18) cause 77.9% of the HR-HPV infections and immunization against type 16 prevents type 31 infections, in this region the efficacy of the prophylactic vaccine against types 16 and 18 would be close to 80%.
Figures
References
-
- Arrossi S, Sankaranarayanan R, Parkin DM. Incidence and mortality of cervical cancer in Latin America. Salud Publica Mex. 2003;45 Suppl 3:S306–14. - PubMed
-
- Reeves WC, Brinton LA, Garcia M, Brenes MM, Herrero R, Gaitan E, Tenorio F, de Britton RC, Rawls WE. Human papillomavirus infection and cervical cancer in Latin America. N Engl J Med. 1989;320:1437–1441. - PubMed
LinkOut - more resources
Full Text Sources
