

Signs and symptoms in diagnosing acute myocardial infarction and acute coronary syndrome: a diagnostic meta-analysis
- PMID: 18307844
- PMCID: PMC2233977
- DOI: 10.3399/bjgp08X277014
Signs and symptoms in diagnosing acute myocardial infarction and acute coronary syndrome: a diagnostic meta-analysis
Abstract
Background: Prompt diagnosis of acute myocardial infarction or acute coronary syndrome is very important.
Aim: A systematic review was conducted to determine the accuracy of 10 important signs and symptoms in selected and non-selected patients.
Design of study: Diagnostic meta-analysis.
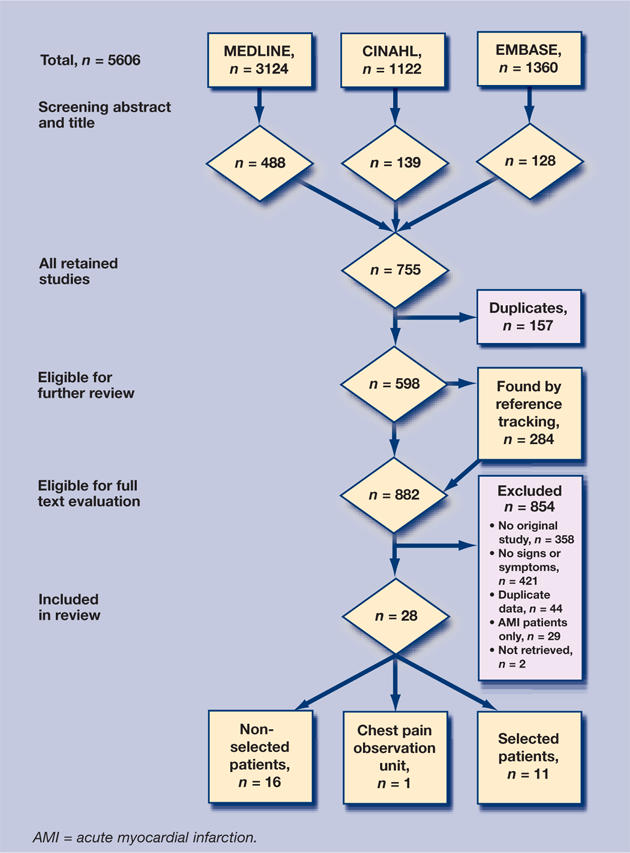
Method: Using MEDLINE, CINAHL, EMBASE, tracing references, and by contacting experts, studies were sought out that described one of the 10 signs and symptoms on one or both conditions. Studies were excluded if they were not based on original data. Validity was assessed using QUADAS and all data were pooled using a random effects model.
Results: Sixteen of the 28 included studies were about patients who were non-selected. In this group, absence of chest-wall tenderness on palpation had a pooled sensitivity of 92% (95% confidence interval [CI] = 86 to 96) for acute myocardial infarction and 94% (95% CI = 91 to 96) for acute coronary syndrome. Oppressive pain followed with a pooled sensitivity of 60% (95% CI = 55 to 66) for acute myocardial infarction. Sweating had the highest pooled positive likelihood ratio (LR+), namely 2.92 (95% CI = 1.97 to 4.23) for acute myocardial infarction. The other pooled LR+ fluctuated between 1.05 and 1.49. Negative LRs (LR-) varied between 0.98 and 0.23. Absence of chest-wall tenderness on palpation had a LR- of 0.23 (95% CI = 0.18 to 0.29).
Conclusions: Based on this meta-analysis it was not possible to define an important role for signs and symptoms in the diagnosis of acute myocardial infarction or acute coronary syndrome. Only chest-wall tenderness on palpation largely ruled out acute myocardial infarction or acute coronary syndrome in low-prevalence settings.
Figures
References
-
- Boersma E, Maas AC, Deckers JW, Simoons M. Early thrombolytic treatment in acute myocardial infarction: re-appraisal of the golden hour. Lancet. 1996;348(9030):771–775. - PubMed
-
- British Heart Foundation. British Heart Foundation Statistics Database. www.heartstats.org (accessed 3 Jan 2008)
-
- Bartholomeeussen S, Truyers C, Buntinx F. Ziekten in de huisartspraktijk in Vlaanderen. [Diseases in General Practices in Flanders.] Leuven: Academisch Centrum voor Huisartsgeneeskunde; 2004.
-
- Buntinx F, Knockaert D, Bruyninckx R, et al. Chest pain in general practice or in the hospital emergency department: is it the same? Fam Pract. 2001;18(6):586–589. - PubMed
-
- Erhardt L, Herlitz J, Bossaert L, et al. Task force on the management of chest pain. Eur Heart J. 2002;23(15):1153–1176. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical