

Neuroprotection for ischemic stroke: past, present and future
- PMID: 18308347
- PMCID: PMC2631228
- DOI: 10.1016/j.neuropharm.2007.12.007
Neuroprotection for ischemic stroke: past, present and future
Abstract
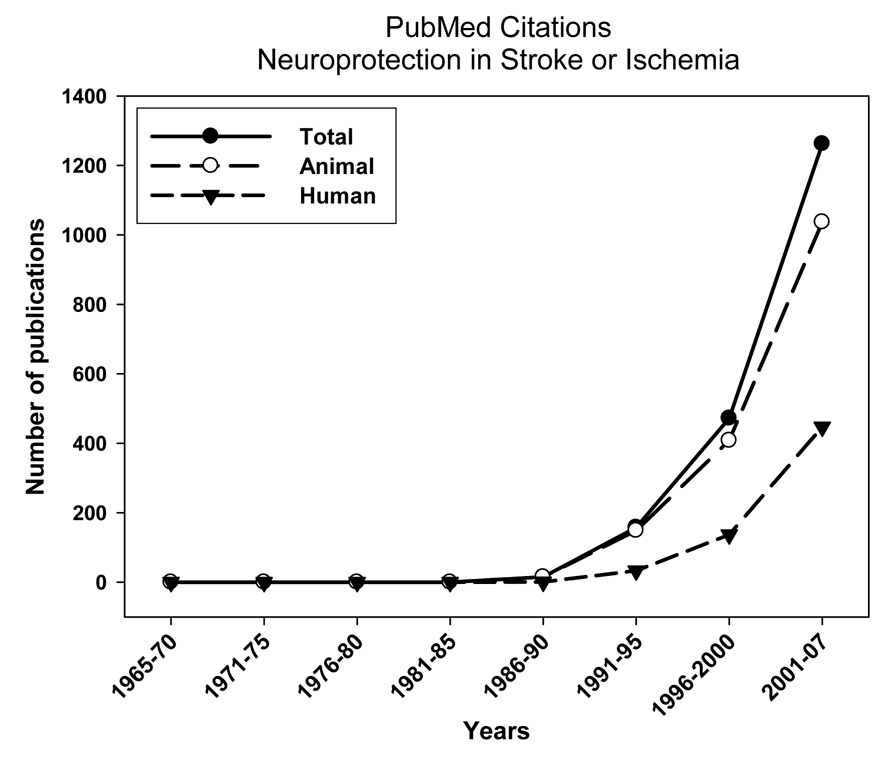
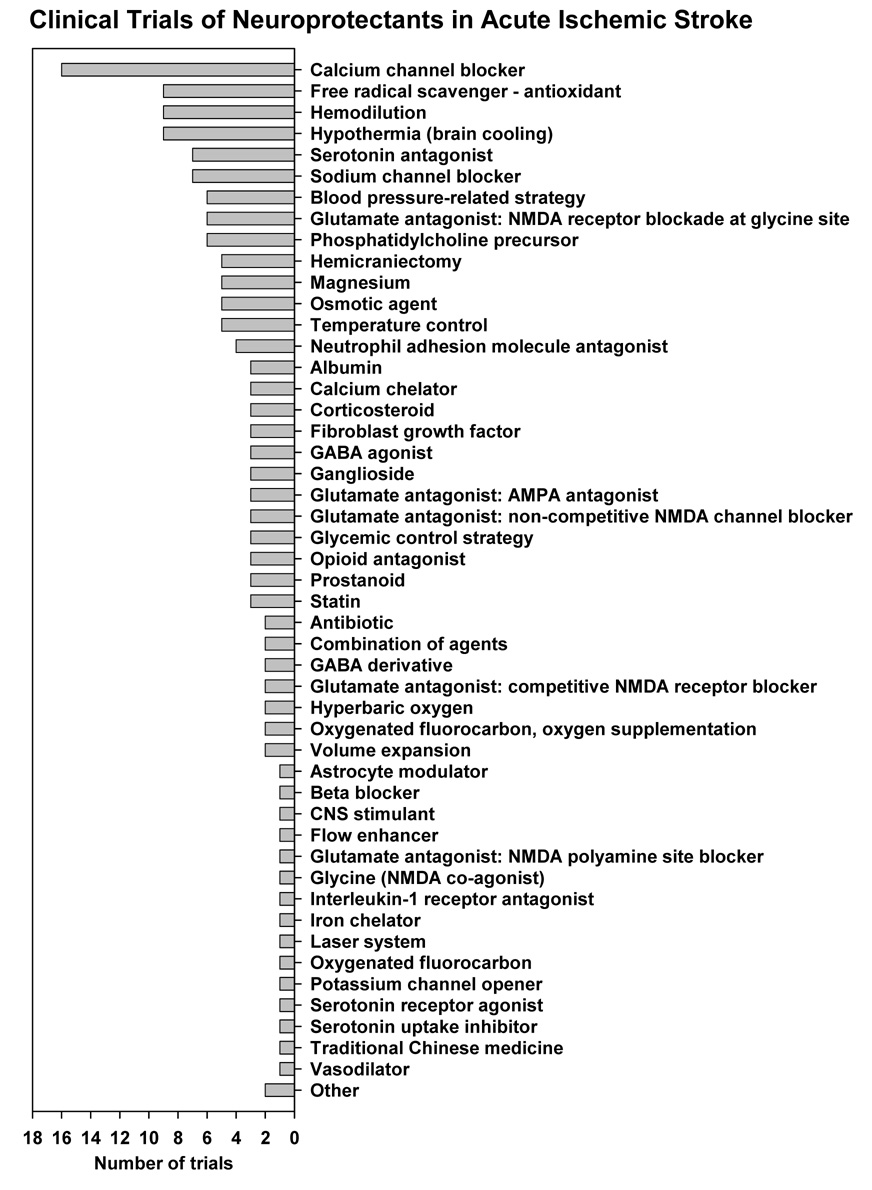
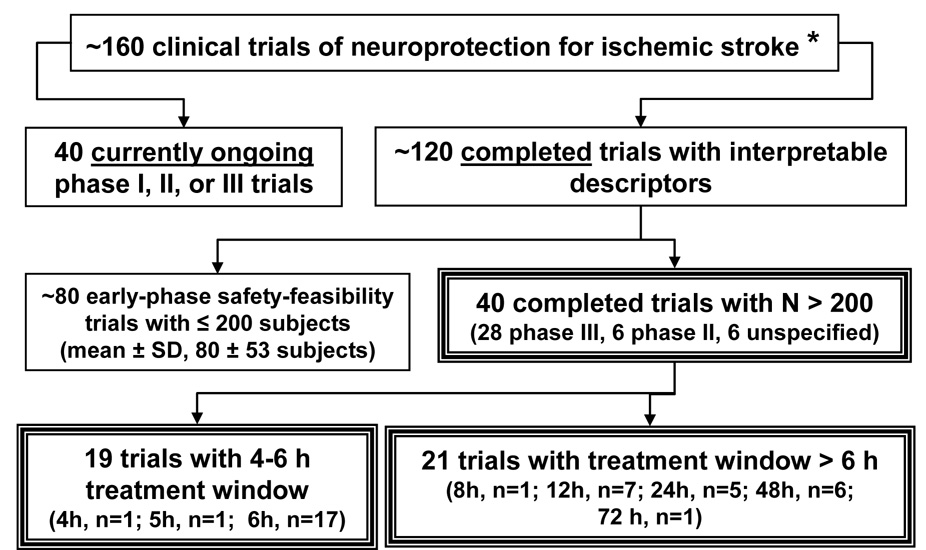
Neuroprotection for ischemic stroke refers to strategies, applied singly or in combination, that antagonize the injurious biochemical and molecular events that eventuate in irreversible ischemic injury. There has been a recent explosion of interest in this field, with over 1000 experimental papers and over 400 clinical articles appearing within the past 6 years. These studies, in turn, are the outgrowth of three decades of investigative work to define the multiple mechanisms and mediators of ischemic brain injury, which constitute potential targets of neuroprotection. Rigorously conducted experimental studies in animal models of brain ischemia provide incontrovertible proof-of-principle that high-grade protection of the ischemic brain is an achievable goal. Nonetheless, many agents have been brought to clinical trial without a sufficiently compelling evidence-based pre-clinical foundation. At this writing, around 160 clinical trials of neuroprotection for ischemic stroke have been initiated. Of the approximately 120 completed trials, two-thirds were smaller early-phase safety-feasibility studies. The remaining one-third were typically larger (>200 subjects) phase II or III trials, but, disappointingly, only fewer than one-half of these administered neuroprotective therapy within the 4-6h therapeutic window within which efficacious neuroprotection is considered to be achievable. This fact alone helps to account for the abundance of "failed" trials. This review presents a close survey of the most extensively evaluated neuroprotective agents and classes and considers both the strengths and weakness of the pre-clinical evidence as well as the results and shortcomings of the clinical trials themselves. Among the agent-classes considered are calcium channel blockers; glutamate antagonists; GABA agonists; antioxidants/radical scavengers; phospholipid precursor; nitric oxide signal-transduction down-regulator; leukocyte inhibitors; hemodilution; and a miscellany of other agents. Among promising ongoing efforts, therapeutic hypothermia, high-dose human albumin therapy, and hyperacute magnesium therapy are considered in detail. The potential of combination therapies is highlighted. Issues of clinical-trial funding, the need for improved translational strategies and clinical-trial design, and "thinking outside the box" are emphasized.
Figures
References
-
- Aarts MM, Tymianski M. Novel treatment of excitotoxicity: targeted disruption of intracellular signalling from glutamate receptors. Biochem. Pharmacol. 2003;66:877–886. - PubMed
-
- Adibhatla RM, Hatcher JF, Dempsey RJ. Phospholipase A2, hydroxyl radicals, and lipid peroxidation in transient cerebral ischemia. Antioxid. Redox. Signal. 2003;5:647–654. - PubMed
-
- Adibhatla RM, Hatcher JF, Larsen EC, Chen X, Sun D, Tsao FH. CDP-choline significantly restores phosphatidylcholine levels by differentially affecting phospholipase A2 and CTP: phosphocholine cytidylyltransferase after stroke. J. Biol. Chem. 2006;281:6718–6725. - PubMed
-
- Aichner FT, Fazekas F, Brainin M, Polz W, Mamoli B, Zeiler K. Hypervolemic hemodilution in acute ischemic stroke: the Multicenter Austrian Hemodilution Stroke Trial (MAHST) Stroke. 1998;29:743–749. - PubMed
-
- Albers GW, Atkinson RP, Kelley RE, Rosenbaum DM. Safety, tolerability, and pharmacokinetics of the N-methyl-D-aspartate antagonist dextrorphan in patients with acute stroke. Dextrorphan Study Group. Stroke. 1995;26:254–258. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
