

Design and end points of clinical trials for patients with progressive prostate cancer and castrate levels of testosterone: recommendations of the Prostate Cancer Clinical Trials Working Group
- PMID: 18309951
- PMCID: PMC4010133
- DOI: 10.1200/JCO.2007.12.4487
Design and end points of clinical trials for patients with progressive prostate cancer and castrate levels of testosterone: recommendations of the Prostate Cancer Clinical Trials Working Group
Abstract
Purpose: To update eligibility and outcome measures in trials that evaluate systemic treatment for patients with progressive prostate cancer and castrate levels of testosterone.
Methods: A committee of investigators experienced in conducting trials for prostate cancer defined new consensus criteria by reviewing previous criteria, Response Evaluation Criteria in Solid Tumors (RECIST), and emerging trial data.
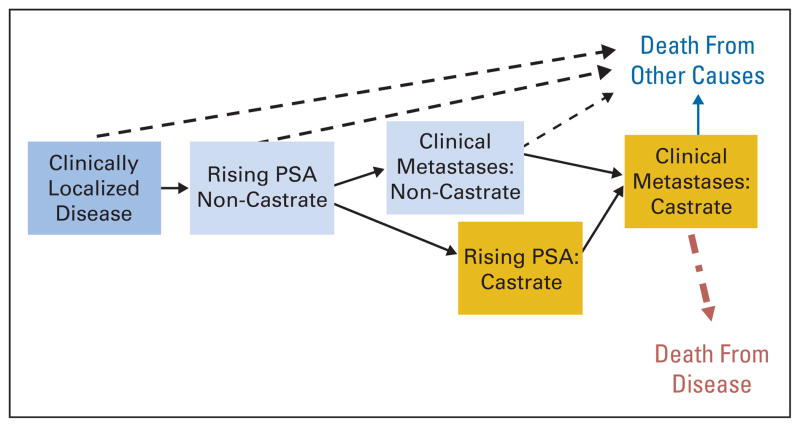
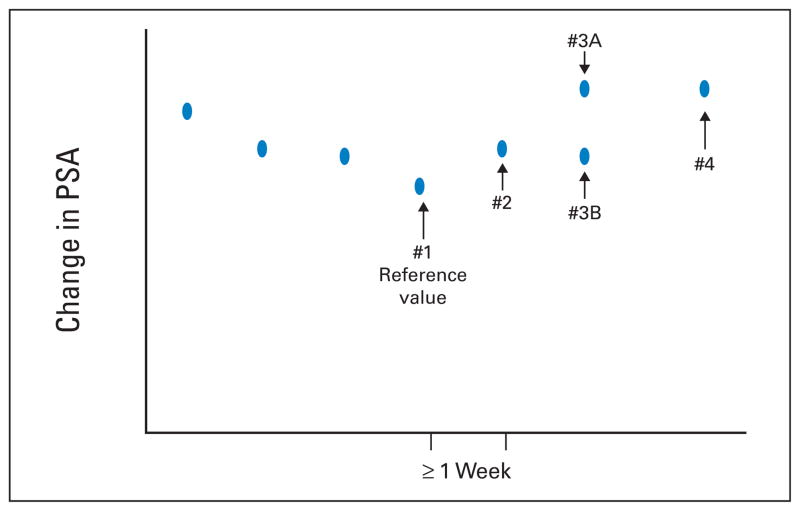
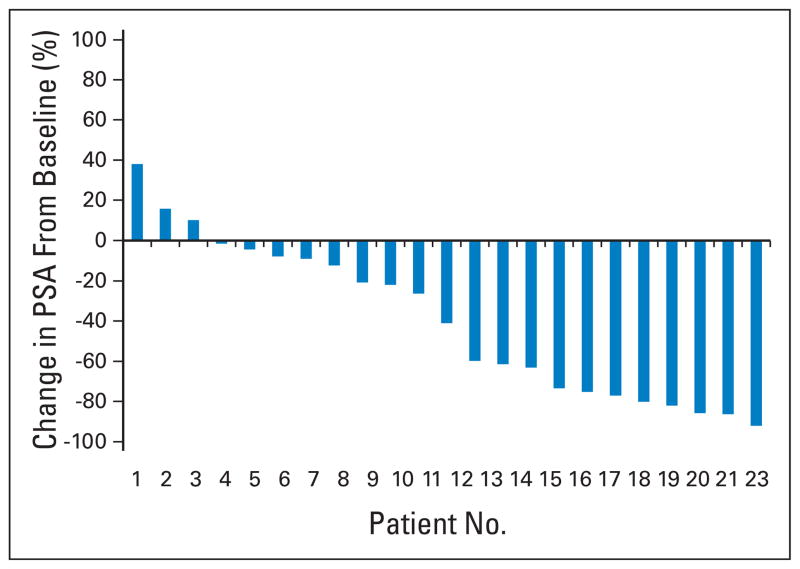
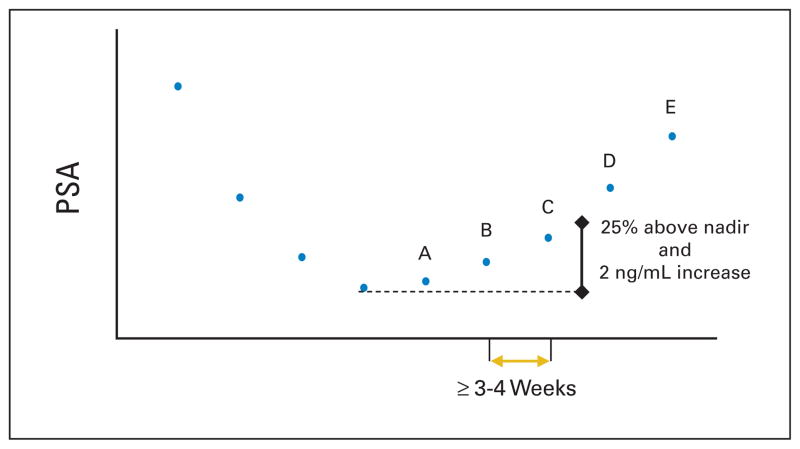
Results: The Prostate Cancer Clinical Trials Working Group (PCWG2) recommends a two-objective paradigm: (1) controlling, relieving, or eliminating disease manifestations that are present when treatment is initiated and (2) preventing or delaying disease manifestations expected to occur. Prostate cancers progressing despite castrate levels of testosterone are considered castration resistant and not hormone refractory. Eligibility is defined using standard disease assessments to authenticate disease progression, prior treatment, distinct clinical subtypes, and predictive models. Outcomes are reported independently for prostate-specific antigen (PSA), imaging, and clinical measures, avoiding grouped categorizations such as complete or partial response. In most trials, early changes in PSA and/or pain are not acted on without other evidence of disease progression, and treatment should be continued for at least 12 weeks to ensure adequate drug exposure. Bone scans are reported as "new lesions" or "no new lesions," changes in soft-tissue disease assessed by RECIST, and pain using validated scales. Defining eligibility for prevent/delay end points requires attention to estimated event frequency and/or random assignment to a control group.
Conclusion: PCWG2 recommends increasing emphasis on time-to-event end points (ie, failure to progress) as decision aids in proceeding from phase II to phase III trials. Recommendations will evolve as data are generated on the utility of intermediate end points to predict clinical benefit.
Conflict of interest statement
Although all authors completed the disclosure declaration, the following author(s) indicated a financial or other interest that is relevant to the subject matter under consideration in this article. Certain relationships marked with a “U” are those for which no compensation was received; those relationships marked with a “C” were compensated. For a detailed description of the disclosure categories, or for more information about ASCO’s conflict of interest policy, please refer to the Author Disclosure Declaration and the Disclosures of Potential Conflicts of Interest section in Information for Contributors.
Figures
Comment in
-
Trial design for metastatic castration-resistant prostate cancer.J Clin Oncol. 2008 Jul 20;26(21):3647-8; author reply 3648-9. doi: 10.1200/JCO.2008.17.1140. J Clin Oncol. 2008. PMID: 18640946 No abstract available.
-
Re: Design and endpoints of clinical trials in patients with progressive prostate cancer and castrate levels of testosterone: recommendations of the Prostate Cancer Clinical Trials Working Group.Eur Urol. 2008 Aug;54(2):462. doi: 10.1016/j.eururo.2008.04.086. Eur Urol. 2008. PMID: 19209432 No abstract available.
-
Castration-resistant prostate cancer: descriptive yet pejorative?J Clin Oncol. 2010 Aug 10;28(23):e408. doi: 10.1200/JCO.2010.28.7664. Epub 2010 Jun 14. J Clin Oncol. 2010. PMID: 20547989 No abstract available.
References
-
- Bubley GJ, Carducci M, Dahut W, et al. Eligibility and response guidelines for phase II clinical trials in androgen-independent prostate cancer: Recommendations from the PSA Working Group. J Clin Oncol. 1999;17:3461–3467. Erratum: J Clin Oncol 18:2644, 2000; J Clin Oncol 25:1154, 2007. - PubMed
-
- Therasse P, Arbuck SG, Eisenhauer EA, et al. New guidelines to evaluate the response to treatment in solid tumors: European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. J Natl Cancer Inst. 2000;92:205–216. - PubMed
-
- Scher HI, Heller G. Clinical states in prostate cancer: Towards a dynamic model of disease progression. Urology. 2000;55:323–327. - PubMed
-
- Simon SD. Is the randomized clinical trial the gold standard of research? J Androl. 2001;22:938–943. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
