

Airway wall thickness assessed using computed tomography and optical coherence tomography
- PMID: 18310475
- PMCID: PMC2408438
- DOI: 10.1164/rccm.200712-1776OC
Airway wall thickness assessed using computed tomography and optical coherence tomography
Abstract
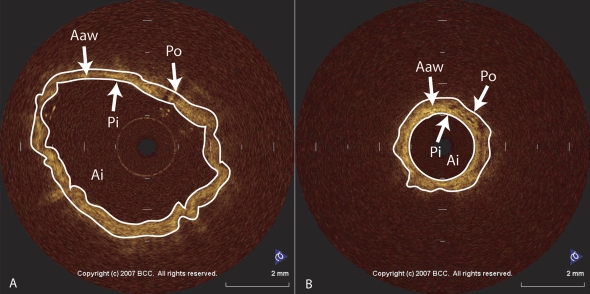
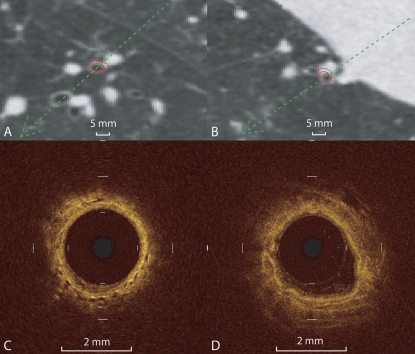
Rationale: Computed tomography (CT) has been shown to reliably measure the airway wall dimensions of medium to large airways. Optical coherence tomography (OCT) is a promising new micron-scale resolution imaging technique that can image small airways 2 mm in diameter or less.
Objectives: To correlate OCT measurements of airway dimensions with measurements assessed using CT scans and lung function.
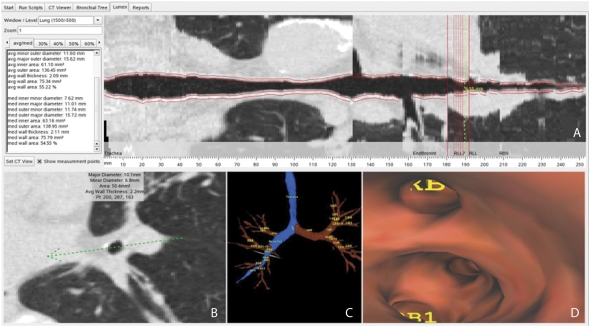
Methods: Forty-four current and former smokers received spirometry, CT scans, and OCT imaging at the time of bronchoscopy. Specific bronchial segments were identified and measured using the OCT images and three-dimensional reconstructions of the bronchial tree using CT.
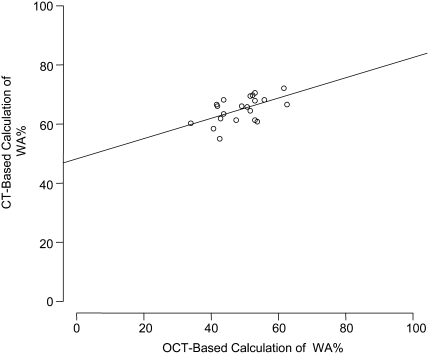
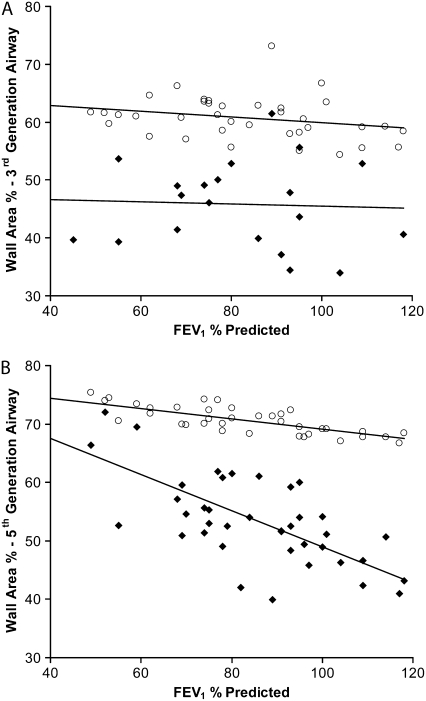
Measurements and main results: There was a strong correlation between CT and OCT measurements of lumen and wall area (r = 0.84, P < 0.001, and r = 0.89, P < 0.001, respectively). Compared with CT, OCT measurements were lower for both lumen and wall area by 31 and 66%, respectively. The correlation between FEV(1)% predicted and CT and OCT measured wall area (as percentage of the total area) of fifth-generation airways was very strong (r = -0.79, r = -0.75), but the slope of the relationship was much steeper using OCT than using CT (y = -0.33x + 82, y = -0.1x + 78), indicating greater sensitivity of OCT in detecting changes in wall measurements that relate to FEV(1).
Conclusions: OCT can be used to measure airway wall dimensions. OCT may be more sensitive at detecting small airway wall changes that lead to FEV(1) changes in individuals with obstructive airway disease.
Figures
References
-
- Celli BR, Snider GL, Heffner J, Tiep B, Ziment I, Make B, Braman S, Olsen G, Phillips Y; Committee of the Scientific Assembly on Clinical Problems. Standards for the diagnosis and care of patients with chronic obstructive pulmonary disease. American Thoracic Society statement. Am J Respir Crit Care Med 1995;152:S77–S120. - PubMed
-
- Pauwels RA, Buist AS, Calverley PM, Jenkins CR, Hurd SS. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. NHLBI/WHO Global Initiative for Chronic Obstructive Lung Disease (GOLD) workshop summary. Am J Respir Crit Care Med 2001;163:1256–1276. - PubMed
-
- Hogg JC, Chu F, Utokaparch S, Woods R, Elliott WM, Buzatu L, Cherniack RM, Rogers RM, Sciurba FC, Coxson HO, et al. The nature of small-airway obstruction in chronic obstructive pulmonary disease. N Engl J Med 2004;350:2645–2653. - PubMed
-
- Hogg JC, Macklem PT, Thurlbeck WM. Site and nature of airway obstruction in chronic obstructive lung disease. N Engl J Med 1968;278:1355–1360. - PubMed
-
- de Jong PA, Muller NL, Pare PD, Coxson HO. Computed tomographic imaging of the airways: relationship to structure and function. Eur Respir J 2005;26:140–152. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
