

Human immunodeficiency virus (HIV) infects human arterial smooth muscle cells in vivo and in vitro: implications for the pathogenesis of HIV-mediated vascular disease
- PMID: 18310503
- PMCID: PMC2276423
- DOI: 10.2353/ajpath.2008.070457
Human immunodeficiency virus (HIV) infects human arterial smooth muscle cells in vivo and in vitro: implications for the pathogenesis of HIV-mediated vascular disease
Abstract
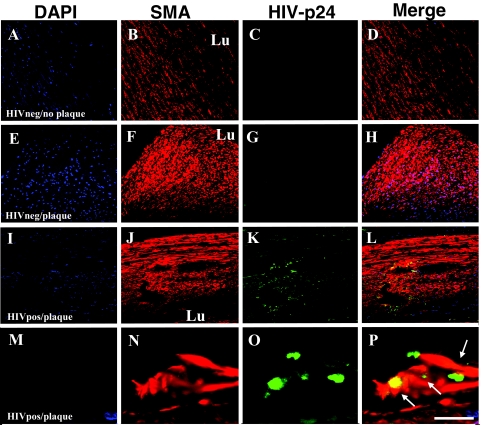
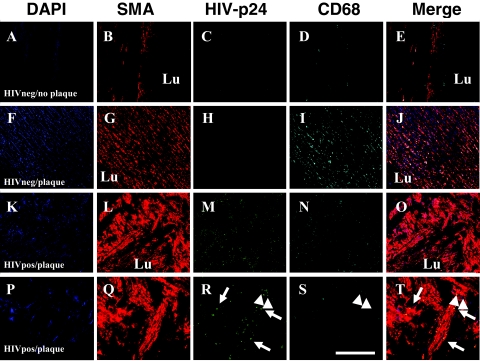
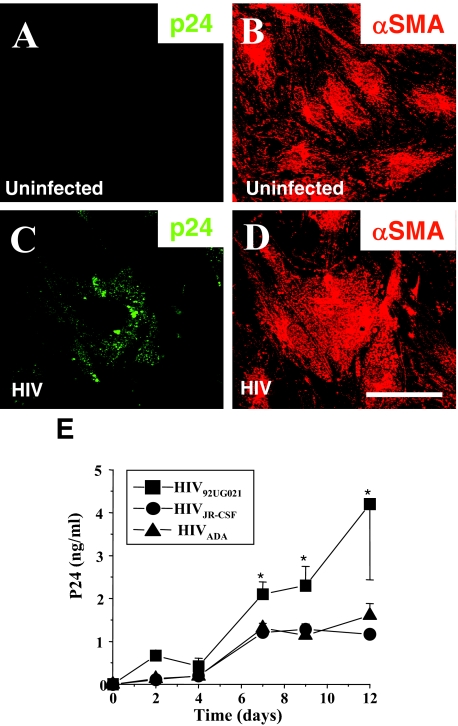
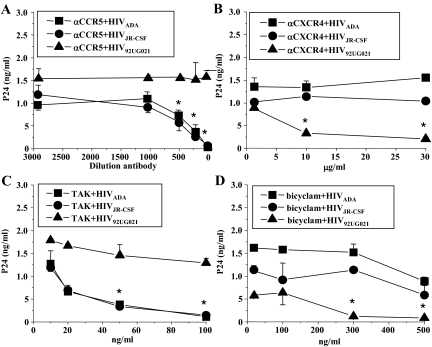
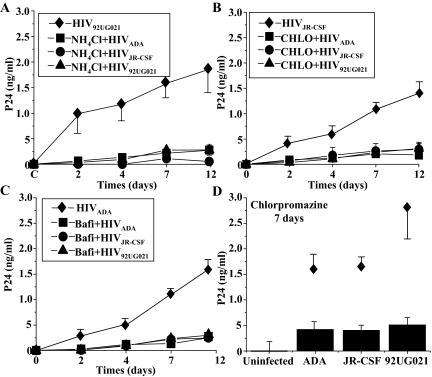
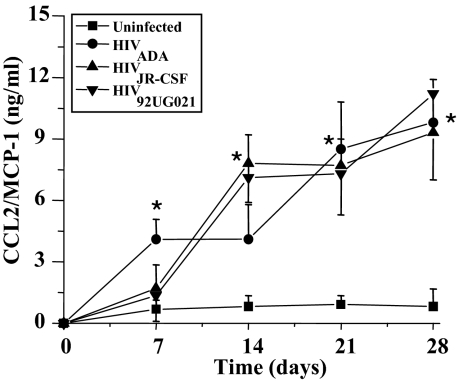
Human immunodeficiency virus (HIV) infection is associated with accelerated atherosclerosis and vasculopathy, although the mechanisms underlying these findings have not been determined. Hypotheses for these observations include: 1) an increase in the prevalence of established cardiac risk factors observed in HIV-infected individuals who are currently experiencing longer life expectancies; 2) the dyslipidemia reported with certain HIV anti-retroviral therapies; and/or 3) the proinflammatory effects of infiltrating HIV-infected monocytes/macrophages. An unexplored possibility is whether HIV itself can infect vascular smooth muscle cells (SMCs) and, by doing so, whether SMCs can accelerate vascular disease. Our studies demonstrate that human SMCs can be infected with HIV both in vivo and in vitro. The HIV protein p24 was detected by fluorescence confocal microscopy in SMCs from tissue sections of human atherosclerotic plaques obtained from HIV-infected individuals. Human SMCs could also be infected in vitro with HIV by a mechanism dependent on CD4, the chemokine receptors CXCR4 or CCR5, and endocytosis, resulting in a marked increase in SMC secretion of the chemokine CCL2/MCP-1, which has been previously shown to be a critical mediator of atherosclerosis. In addition, SMC proliferation appeared concentric to the vessel lumen, and minimal inflammation was detected, unlike typical atherosclerosis. Our data suggest that direct infection of human arterial SMCs by HIV represents a potential mechanism in a multifactorial paradigm to explain the exacerbated atherosclerosis and vasculopathy reported in individuals infected with HIV.
Figures

References
-
- Bokazhanova A, Rutherford GW. The epidemiology of HIV and AIDS in the world. Coll Antropol. 2006;30(Suppl 2):3–10. - PubMed
-
- de Saint Martin L, Vandhuick O, Guillo P, Bellein V, Bressollette L, Roudaut N, Amaral A, Pasquier E. Premature atherosclerosis in HIV positive patients and cumulated time of exposure to antiretroviral therapy (SHIVA study). Atherosclerosis. 2006;185:361–367. - PubMed
-
- Hsue PY, Giri K, Erickson S, MacGregor JS, Younes N, Shergill A, Waters DD. Clinical features of acute coronary syndromes in patients with human immunodeficiency virus infection. Circulation. 2004;109:316–319. - PubMed
-
- Segev A, Cantor WJ, Strauss BH. Outcome of percutaneous coronary intervention in HIV-infected patients. Catheter Cardiovasc Interv. 2006;68:879–881. - PubMed
-
- van Wijk JP, de Koning EJ, Cabezas MC, Joven J, op’t Roodt J, Rabelink TJ, Hoepelman AM. Functional and structural markers of atherosclerosis in human immunodeficiency virus-infected patients. J Am Coll Cardiol. 2006;47:1117–1123. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U24 MH100931/MH/NIMH NIH HHS/United States
- P30 AI051519/AI/NIAID NIH HHS/United States
- MH 052974/MH/NIMH NIH HHS/United States
- R01 MH070297/MH/NIMH NIH HHS/United States
- U01 MH083501/MH/NIMH NIH HHS/United States
- K01 MH076679/MH/NIMH NIH HHS/United States
- P50 NS011920/NS/NINDS NIH HHS/United States
- K01 MH 076679/MH/NIMH NIH HHS/United States
- R24 MH059724/MH/NIMH NIH HHS/United States
- MH 075679/MH/NIMH NIH HHS/United States
- R24 MH 59724/MH/NIMH NIH HHS/United States
- MH 070297/MH/NIMH NIH HHS/United States
- NS 11920/NS/NINDS NIH HHS/United States
- AI 051519/AI/NIAID NIH HHS/United States
- R01 HL 7458/HL/NHLBI NIH HHS/United States
- R01 MH075679/MH/NIMH NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
