

Autoantibodies and neuropsychiatric events at the time of systemic lupus erythematosus diagnosis: results from an international inception cohort study
- PMID: 18311802
- PMCID: PMC4656035
- DOI: 10.1002/art.23218
Autoantibodies and neuropsychiatric events at the time of systemic lupus erythematosus diagnosis: results from an international inception cohort study
Abstract
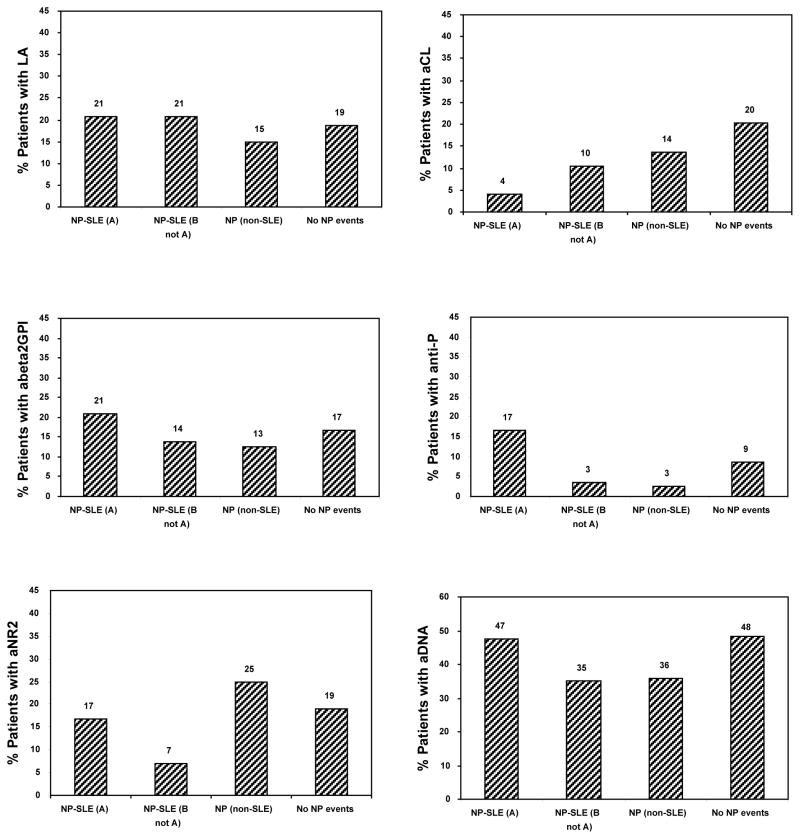
Objective: To examine, in an inception cohort of systemic lupus erythematosus (SLE) patients, the association between neuropsychiatric (NP) events and anti-ribosomal P (anti-P), antiphospholipid (lupus anticoagulant [LAC], anticardiolipin), anti-beta2-glycoprotein I, and anti-NR2 glutamate receptor antibodies.
Methods: NP events were identified using the American College of Rheumatology case definitions and clustered into central/peripheral and diffuse/focal events. Attribution of NP events to SLE was determined using decision rules of differing stringency. Autoantibodies were measured without knowledge of NP events or their attribution.
Results: Four hundred twelve patients were studied (87.4% female; mean +/- SD age 34.9 +/- 13.5 years, mean +/- SD disease duration 5.0 +/- 4.2 months). There were 214 NP events in 133 patients (32.3%). The proportion of NP events attributed to SLE varied from 15% to 36%. There was no association between autoantibodies and NP events overall. However, the frequency of anti-P antibodies in patients with central NP events attributed to SLE was 4 of 20 (20%), versus 3 of 107 (2.8%) in patients with other NP events and 24 of 279 (8.6%) in those with no NP events (P = 0.04). Among patients with diffuse NP events, 3 of 11 had anti-P antibodies (27%), compared with 4 of 111 patients with other NP events (3.6%) and 24 of 279 of those with no NP events (8.6%) (P = 0.02). Specific clinical-serologic associations were found between anti-P and psychosis attributed to SLE (P = 0.02) and between LAC and cerebrovascular disease attributed to SLE (P = 0.038). There was no significant association between other autoantibodies and NP events.
Conclusion: Clinically distinct NP events attributed to SLE and occurring around the time of diagnosis were found to be associated with anti-P antibodies and LAC. This suggests that there are different autoimmune pathogenetic mechanisms, although low sensitivity limits the clinical application of testing for these antibodies.
Figures


References
-
- Ainiala H, Hietaharju A, Loukkola J, et al. Validity of the new American College of Rheumatology criteria for neuropsychiatric lupus syndromes: a population-based evaluation. Arthritis Rheum. 2001;45(5):419–23. - PubMed
-
- Brey RL, Holliday SL, Saklad AR, et al. Neuropsychiatric syndromes in lupus: prevalence using standardized definitions. Neurology. 2002;58(8):1214–20. - PubMed
-
- Hanly JG, McCurdy G, Fougere L, Douglas JA, Thompson K. Neuropsychiatric events in systemic lupus erythematosus: attribution and clinical significance. J Rheumatol. 2004;31(11):2156–62. - PubMed
-
- Sanna G, Bertolaccini ML, Cuadrado MJ, Laing H, Mathieu A, Hughes GR. Neuropsychiatric manifestations in systemic lupus erythematosus: prevalence and association with antiphospholipid antibodies. J Rheumatol. 2003;30(5):985–92. - PubMed
-
- Sibbitt WL, Jr, Brandt JR, Johnson CR, et al. The incidence and prevalence of neuropsychiatric syndromes in pediatric onset systemic lupus erythematosus. J Rheumatol. 2002;29(7):1536–42. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- P60 AR048095/AR/NIAMS NIH HHS/United States
- M01 RR000048/RR/NCRR NIH HHS/United States
- P60 AR048098/AR/NIAMS NIH HHS/United States
- M01-RR-00052/RR/NCRR NIH HHS/United States
- M01 RR000052/RR/NCRR NIH HHS/United States
- WT_/Wellcome Trust/United Kingdom
- AR-43727/AR/NIAMS NIH HHS/United States
- P60-AR-48095/AR/NIAMS NIH HHS/United States
- K24-AR-02318/AR/NIAMS NIH HHS/United States
- P60-AR-48098/AR/NIAMS NIH HHS/United States
- M01-RR-00048/RR/NCRR NIH HHS/United States
- 86526-2/CAPMC/ CIHR/Canada
- R01 AR043727/AR/NIAMS NIH HHS/United States
- ARC_/Arthritis Research UK/United Kingdom
- MC_U105261167/MRC_/Medical Research Council/United Kingdom
- 86526-1/CAPMC/ CIHR/Canada
LinkOut - more resources
Full Text Sources
Miscellaneous
