

Acute lung injury and the acute respiratory distress syndrome in Ireland: a prospective audit of epidemiology and management
- PMID: 18312626
- PMCID: PMC2374618
- DOI: 10.1186/cc6808
Acute lung injury and the acute respiratory distress syndrome in Ireland: a prospective audit of epidemiology and management
Abstract
Introduction: The aim of this study was to describe the epidemiology and management of acute lung injury (ALI) and the acute respiratory distress syndrome (ARDS) in Ireland.
Methods: As part of a 10-week prospective national audit of patient demographics and organ failure incidence in intensive care in Ireland, all patients with ALI/ARDS in 14 participating centres were prospectively identified using American European Consensus Conference definitions.
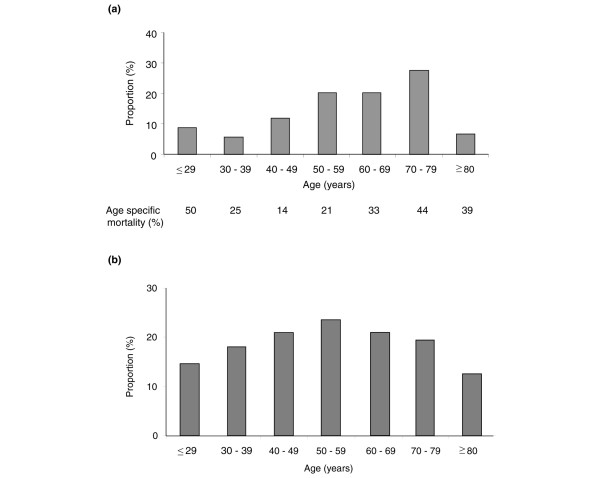
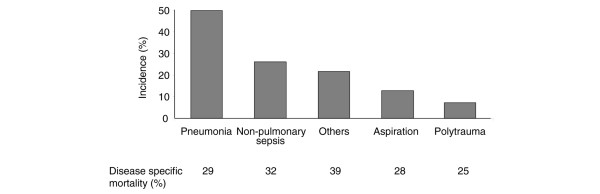
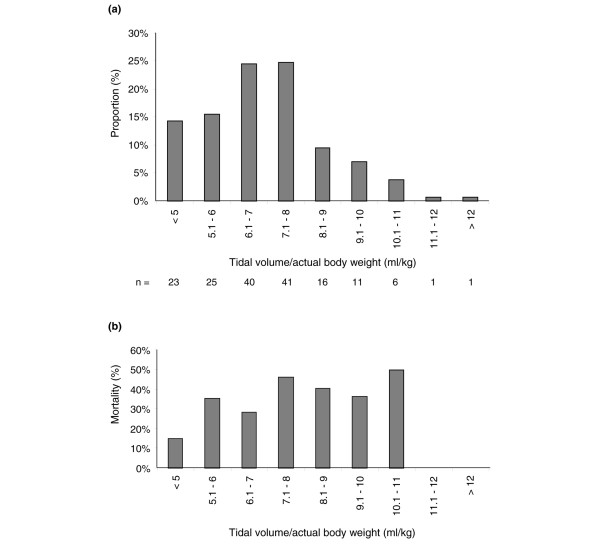
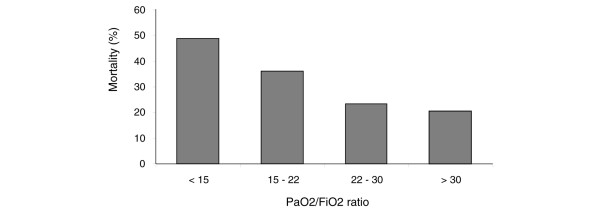
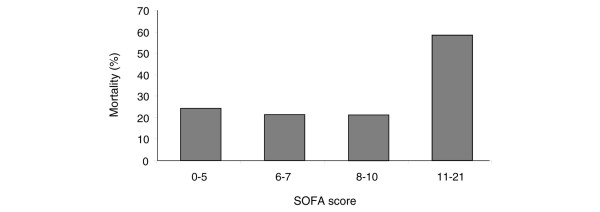
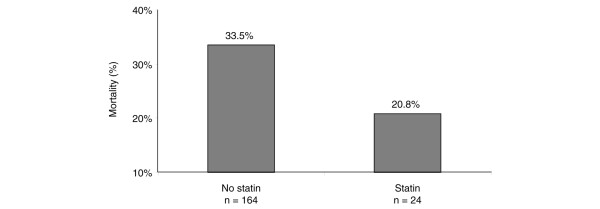
Results: There were 1,029 admissions during the study period; of these, 728 patients were invasively ventilated. A total of 196 (19%) patients had ALI/ARDS, and 141 of these (72%) had ALI/ARDS on admission and a further 55 (28%) developed ALI/ARDS after admission. For the patients with ALI/ARDS, the mean (+/- standard deviation) age was 58 +/- 17 years and 62% were male. The most common predisposing risk factors were pneumonia (50%) and nonpulmonary sepsis (26%). Mean (+/- standard deviation) tidal volume/kg was 7.0 +/- 1.7 ml/kg. Median (interquartile range) duration of ventilation was 6.8 (2.0 to 12.8) days. Median (interquartile range) length of stay in the intensive care unit was 10.0 (5.0 to 18.5) days. The overall intensive care unit mortality for ALI/ARDS was 32.3%. Lower baseline arterial oxygen tension/fraction of inspired oxygen ratio and higher Sequential Organ Failure Assessment scores were associated with increased mortality. Although not significant, patients receiving treatment with a statin during admission had a 73% lower odds of death (odds ratio 0.27, 95% confidence interval 0.06 to 1.21; P = 0.09).
Conclusion: The incidence of ALI/ARDS is high and is associated with significant mortality. Protective lung ventilation is used commonly throughout participating centres. With low tidal volume ventilation, the degree of hypoxaemia is associated with outcome. These data will inform future multicentre clinical trials in ALI/ARDS in Ireland.
Figures
Comment in
-
Lost in translation? The pursuit of lung-protective ventilation.Crit Care. 2008;12(2):122. doi: 10.1186/cc6828. Epub 2008 Mar 31. Crit Care. 2008. PMID: 18423069 Free PMC article.
References
-
- Unit Costs of Health and Social Care http://www.pssru.ac.uk/pdf/uc2004/uc2005_s07.pdf
-
- Craig T, O'Kane CM, McAuley DF. Potential mechanisms by which statins modulate pathogenic mechanisms important in the development of acute lung injury. In: Vincent JL, editor. 27th Yearbook of Intensive Care and Emergency Medicine. Berlin, Germany: Springer-Verlag; 2007. pp. 287–300.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
