

Review
doi: 10.1016/j.hfc.2007.10.004.
The cardiac cycle and the physiologic basis of left ventricular contraction, ejection, relaxation, and filling
Affiliations
- PMID: 18313620
- PMCID: PMC2390899
- DOI: 10.1016/j.hfc.2007.10.004
Item in Clipboard
Review
The cardiac cycle and the physiologic basis of left ventricular contraction, ejection, relaxation, and filling
Heart Fail Clin.
2008 Jan.
Abstract
Heart failure is defined as the pathologic state in which the heart is unable to pump blood at a rate required by the metabolizing tissues or can do so only with an elevated filling pressure. Heart failure in adults most frequently results from the inability of the left ventricle to fill (diastolic performance) or eject (systolic performance) blood. The severity of heart failure and its prognosis are more closely related to the degree of diastolic filling abnormalities than the ejection fraction, which underscores the importance of understanding the mechanisms of diastolic abnormalities in heart failure.
Figures
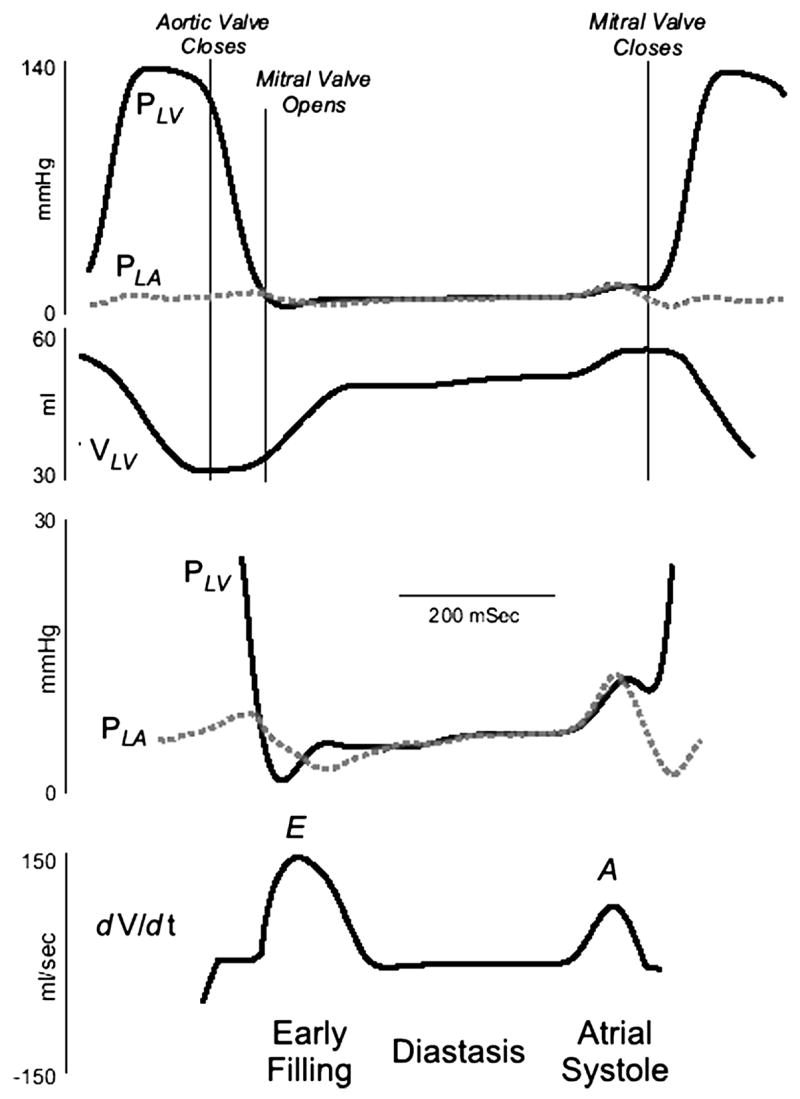
Recording of left atrial pressure (PLA), left ventricular pressure (PLV), and the rate of change of left ventricular (LV) volume (dV/dt). The early diastolic pressure gradient is generated as LV pressure falls below LA pressure and the late diastolic gradient is generated as atrial contraction increases LA pressure above LV pressure. Data from Little WC, Cheng CP. Left ventricular-arterial coupling in conscious dogs. Am J Physiol 1991;261:H70–H76.
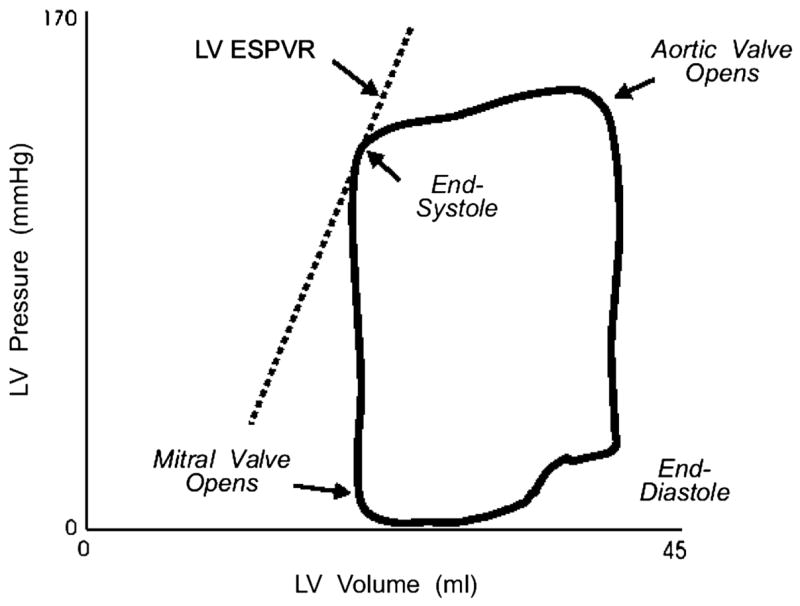
A left ventricular (LV) pressure-volume loop, describing one cardiac cycle. ESPVR indicates the end-systolic pressure-volume relation. See text for discussion. Data from Little WC, Cheng CP. Left ventricular-arterial coupling in conscious dogs. Am J Physiol 1991;261:H70–H76.
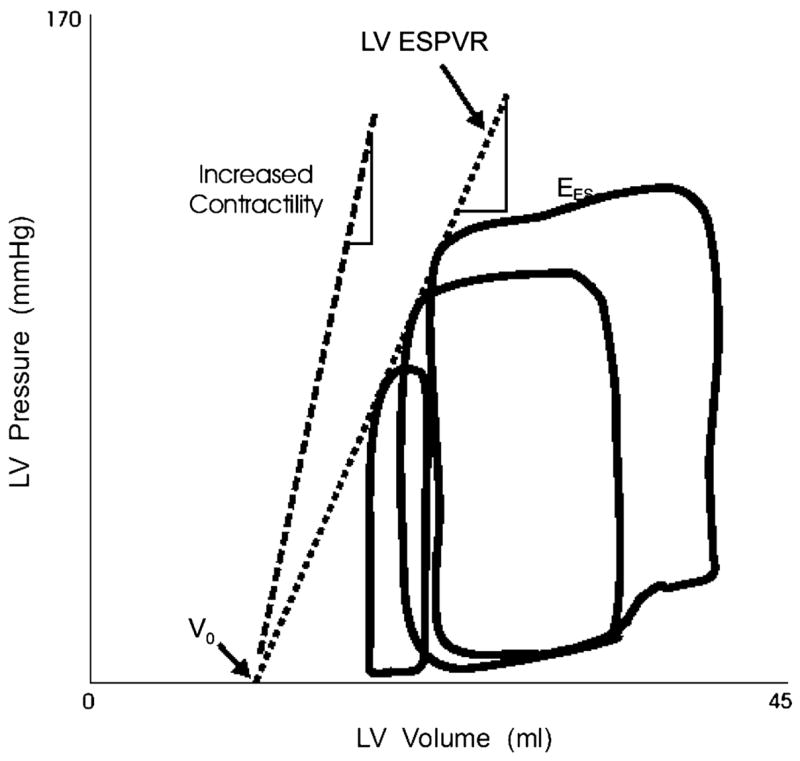
Variably loaded pressure-volume loops produced by caval occlusion are shown. End systole occurs at the upper left corner of the pressure-volume loops. The end-systolic points of variably loaded beats fall along a single relation, the left ventricular end-systolic pressure-volume relation (LV ESPVR). Within the physiological range, this relation is approximately by a straight line. The line can be described in terms of its slope (Ees) and volume axis intercept (Vo). Data from Little WC, Cheng CP, Mumma M, Igarashi Y, Vinten-Johansen J, Johnston WE. Comparison of measures of left ventricular contractile performance derived from pressure-volume loops in conscious dogs. Circulation 1989;80:1378–1387.
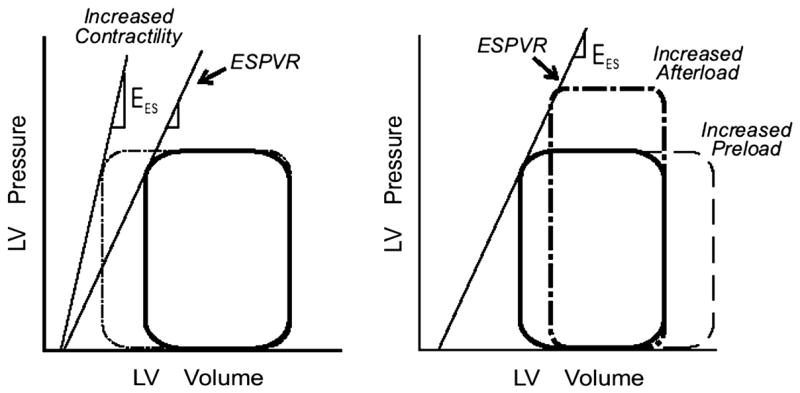
The responses of the left ventricle (LV) to increases in afterload and preload and contractility in the pressure-volume plane. LV ESPVR, the left ventricular end-systolic pressure-volume relation; Ees, the slope of the end-systolic pressure-volume relation. See text for discussion. Adapted from Little WC. Assessment of normal and abnormal cardiac function. In: Braunwald, Zipes, Libby, eds. Heart disease: A textbook of cardiovascular medicine. 6 ed. Philadelphia: W.B. Saunders Company; 2001:479–502.
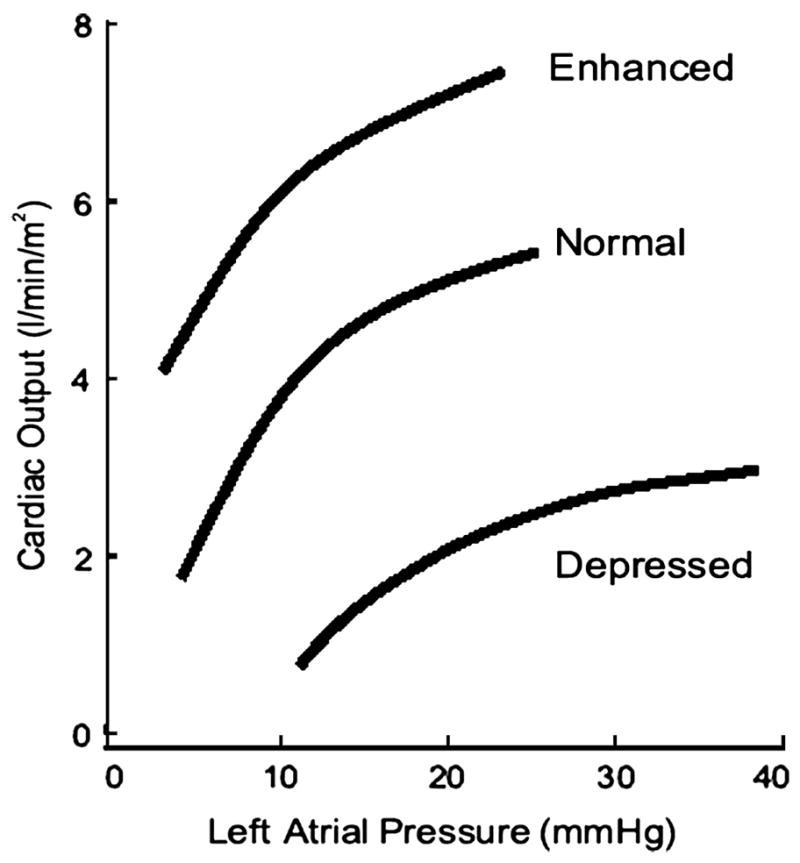
The Starling relationship. With increasing left ventricular filling pressure measured by the pulmonary capillary wedge pressure, there is an increase in cardiac output. The positions of the curves are influenced by the contractile state of the left ventricle. Adapted from Little WC. Assessment of normal and abnormal cardiac function. In: Braunwald, Zipes, Libby, eds. Heart disease: A textbook of cardiovascular medicine. 6 ed. Philadelphia: W.B. Saunders Company; 2001:479–502.
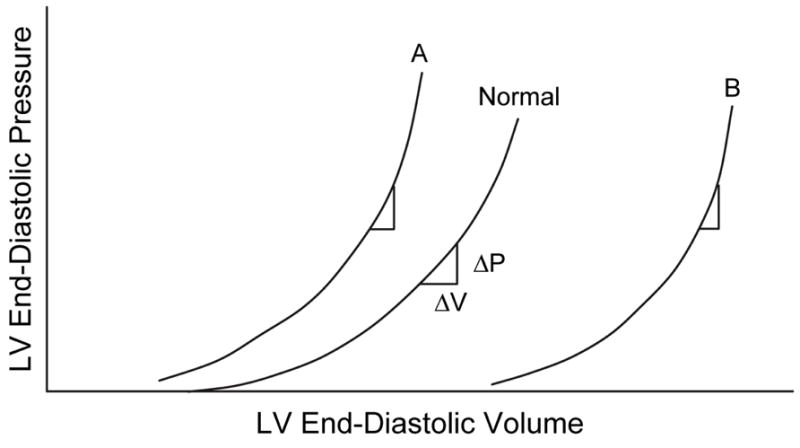
A shift of the curve to A indicates that a higher left ventricular (LV) pressure will be required to distend the LV to a similar volume, indicating that the ventricle is less distensible. The slope of the LV end-diastolic pressure-volume relation indicates the passive chamber stiffness. Since the relation is exponential in shape, the slope (ΔP/ΔV) increases as the end-diastolic pressure increases. From Little WC. Diastolic dysfunction beyond distensibility: adverse effects of ventricular dilatation. Circulation 2005;112:2888–2890.
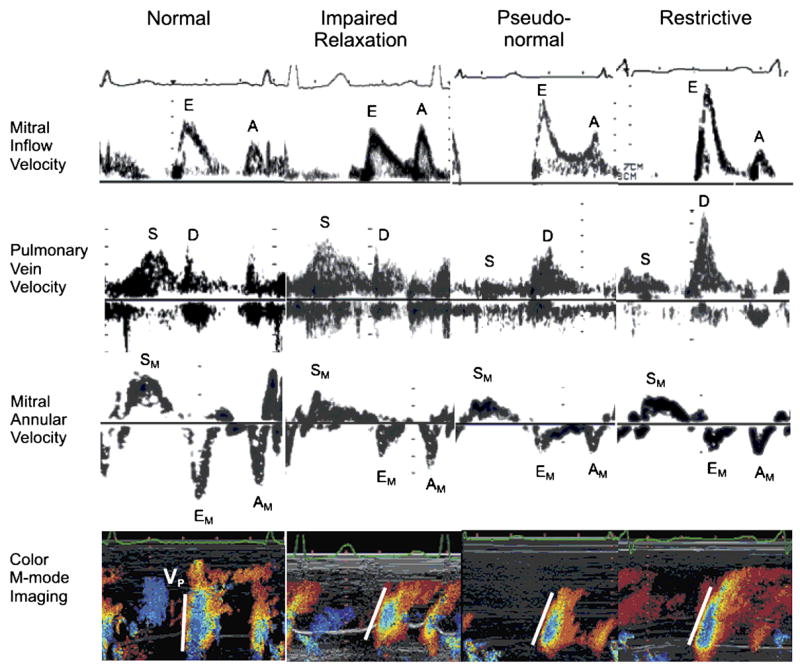
Transmitral inflow velocity, pulmonary vein flow velocity, mitral annular velocity, and color M-mode imaging in stages of diastolic dysfunction. E indicates early diastolic mitral inflow velocity; A, late diastolic mitral inflow velocity; S, systolic pulmonary vein velocity; D, diastolic pulmonary vein velocity; SM, systolic mitral annular velocity; EM, early diastolic mitral annular velocity; AM, late diastolic mitral annular velocity; and Vp, velocity of propagation of mitral inflow to the apex. Reprinted with permission. From Fukuta H, Little WC. Contribution of systolic and diastolic abnormalities to heart failure with a normal and a reduced ejection fraction. Prog Cardiovasc Dis 2007;49:229–240.
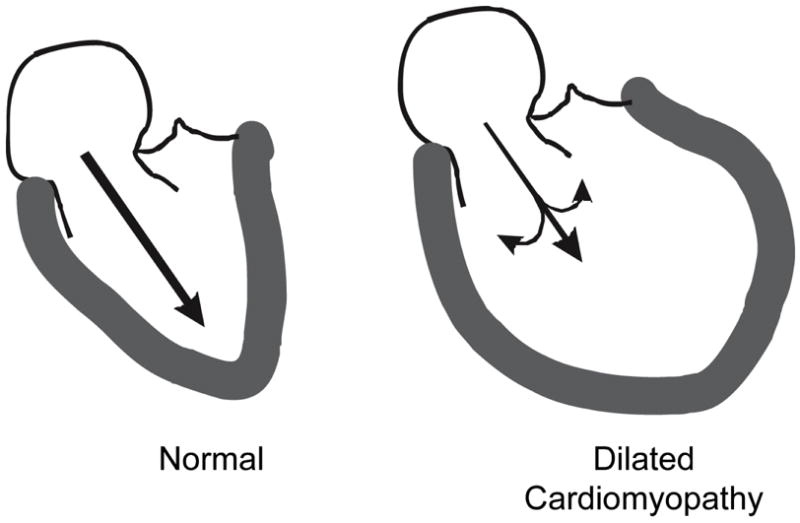
Diagram of the early diastolic left ventricular (LV) filling. In the normal heart, recoil of elastic elements produces a progressive pressure gradient from the left atrium to the apex of the left ventricle. This results in acceleration of blood from the left atrium to the LV apex, resulting in rapid diastolic filling. In a patient with a dilated cardiomyopathy, there is less elastic recoil. The acceleration of blood to the apex is further reduced by convective deceleration which is the tendency for blood to diverge from the longitudinal axis forming vortices in the dilated ventricle. Reprinted with permission. From Little WC. Diastolic dysfunction beyond distensibility: adverse effects of ventricular dilatation. Circulation 2005;112:2888–2890.
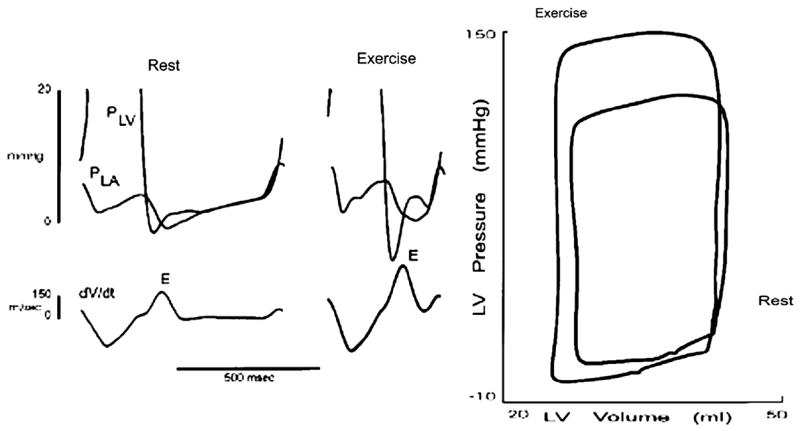
Recording of left atrial pressure (PLA), left ventricular pressure (PLV), and the rate of change of left ventricular (LV) volume (dV/dt) in a conscious animal at rest and during exercise. The data are also shown in the pressure-volume plane. See text for discussion. Data from Cheng CP, Igarashi Y, Little WC. Mechanism of augmented rate of left ventricle filling during exercise. Circ Res 1992;70:9–19.
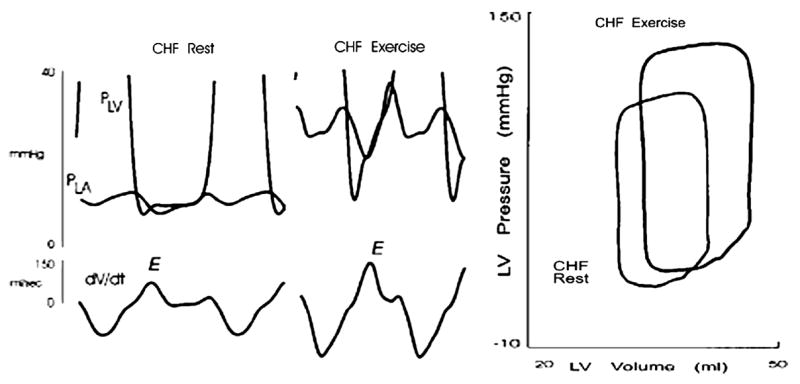
Recording from the same animal as in Figure 9 after the induction of pacing-induced heart failure (CHF). The data are also shown in the pressure-volume plane. See text for discussion. Data from Cheng CP, Noda T, Nozawa T, Little WC. Effect of heart failure on the mechanism of exercise-induced augmentation of mitral valve flow. Circ Res 1993;72:795–806.
References
-
- Brutsaert DL, De Keulenaer GW. Diastolic heart failure: a myth. Curr Opin Cardiol. 2006;21:240–248. - PubMed
-
- Little WC. Assessment of normal and abnormal cardiac function. In: Braunwald, Zipes, Libby, editors. Heart disease: A text book of cardiovascular medicine. 6. Philadelphia: W.B. Saunders Company; 2001. pp. 479–502.
-
- Little WC, Applegate RJ. Congestive heart failure: systolic and diastolic function. J Cardiothorac Vasc Anesth. 1993;7:2–5. - PubMed
-
- Little WC. Diastolic dysfunction beyond distensibility: adverse effects of ventricular dilatation. Circulation. 2005;112:2888–2890. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
