

Review
doi: 10.1016/j.hfc.2007.10.001.
Ventricular-vascular interaction in heart failure
Affiliations
- PMID: 18313622
- PMCID: PMC2586173
- DOI: 10.1016/j.hfc.2007.10.001
Item in Clipboard
Review
Ventricular-vascular interaction in heart failure
Heart Fail Clin.
2008 Jan.
Abstract
Nearly half of all patients who have heart failure have preserved ejection fraction (HFpEF). Patients who have HFpEF tend to be older, female, and hypertensive, and characteristically display increased ventricular and arterial stiffening. In this article, we discuss the pathophysiology of abnormal ventriculoarterial stiffening and how it affects ventricular function, cardiovascular hemodynamics, reserve capacity, and symptoms. We conclude by exploring how novel treatment strategies targeting abnormal ventricular-arterial interaction might prove useful in the treatment of patients who have HFpEF.
Figures
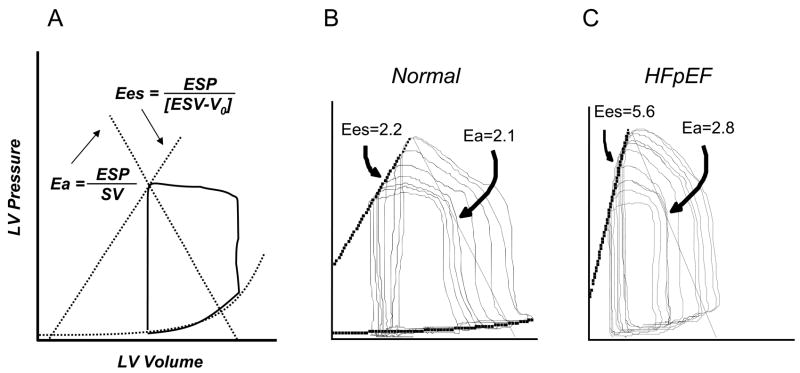
[A] Left ventricular end systolic elastance (Ees) is described by the slope and intercept of the end-systolic pressure-volume relationship, while arterial elastance (Ea) is defined by the negative slope between the end-systolic pressure volume point and end diastolic volume. [B] A normal adult has relatively low Ees and Ea, with a coupling ratio around unity, while older aged, hypertensive and HFpEF subjects [C] display marked increases in ventricular and arterial elastance.
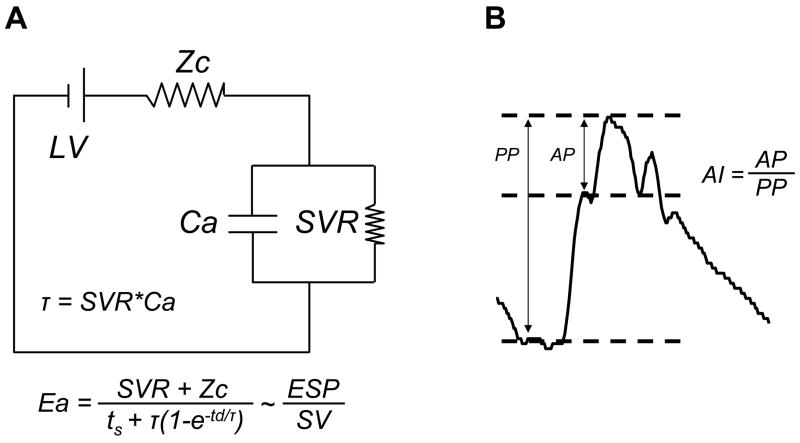
Effective arterial elastance incorporates both mean resistive and pulsatile components of afterload. Panel [A] shows the electrical circuit analog of the 3-element Windkessel model, which consists of a proximal characteristic impedance (Zc) upstream of total arterial compliance (Ca) and systemic vascular resistance (SVR) arranged in parallel. [B] With vascular stiffening, pulse wave velocity increases, such that reflected waves return to the ascending aorta in late systole rather than early diastole. The magnitude of late-systolic load can then be quantified by the augmentation index (AI), described by the ratio of augmented (AP) to pulse pressure (PP).
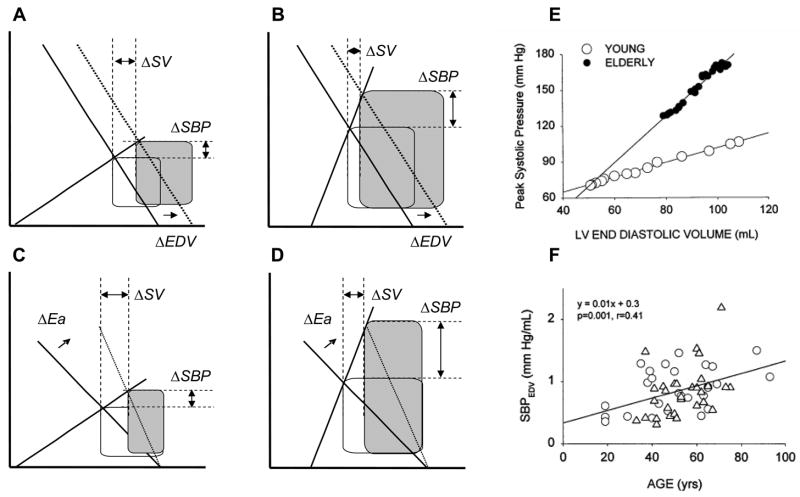
[A] Isolated increases in preload volume (EDV) with stable Ees and Ea lead to increases in blood pressure (BP) and stroke volume, but in a stiff ventriculoarterial system [B], the same increase in EDV produces a much larger increase in BP with proportionately less augmentation in stroke volume. Similarly, an isolated increase in afterload produces much more increase in BP in a stiff system [D] compared with normal or low elastances [C]. Note again that the change in stroke volume is much less pronounced in the stiff heart-artery system, and the stroke work or pressure-volume area (shaded) is much greater, indicating higher myocardial oxygen demand to achieve the same net volume transfer. Increased stiffness explains why older adults show much greater dependence of BP on preload [E]. The slope of the SBP-preload relation is higher in healthy older versus younger subjects [F]. Panels E and F from Chen CH, Nakayama M, Nevo E, Fetics BJ, Maughan WL, Kass DA. Coupled systolic-ventricular and vascular stiffening with age: implications for pressure regulation and cardiac reserve in the elderly. J Am Coll Cardiol. Nov 1998;32(5):1221–1227.
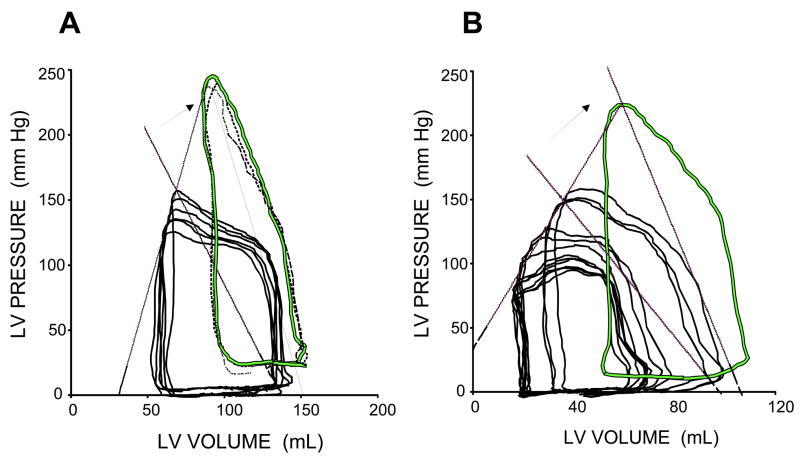
Example pressure volume loops taken from patients with HFpEF at baseline and with acute increases in Ea induced by isometric handgrip (arrows). Because of elevated baseline stiffness, the “gain” is much greater with further increases, leading to severe hypertension. Note the greatly increased end-diastolic LV pressures during handgrip. From Kawaguchi M, Hay I, Fetics B, Kass DA. Combined ventricular systolic and arterial stiffening in patients with heart failure and preserved ejection fraction: implications for systolic and diastolic reserve limitations. Circulation. Feb 11 2003;107(5):714–720.
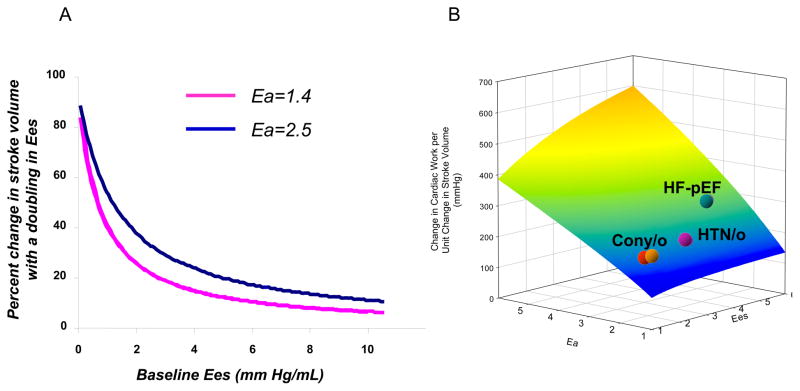
[A] Starting from a high resting ventricular stiffness greatly limits the capability of the cardiovascular system to further increase stroke volume, regardless of baseline Ea. [B] Energetic costs are highest in HFpEF patients to augment stroke work because of increased Ea and Ees, decreasing efficiency and potentially predisposing to ischemia. Panel 5B from Kawaguchi M, Hay I, Fetics B, Kass DA. Combined ventricular systolic and arterial stiffening in patients with heart failure and preserved ejection fraction: implications for systolic and diastolic reserve limitations. Circulation. Feb 11 2003;107(5):714–720.
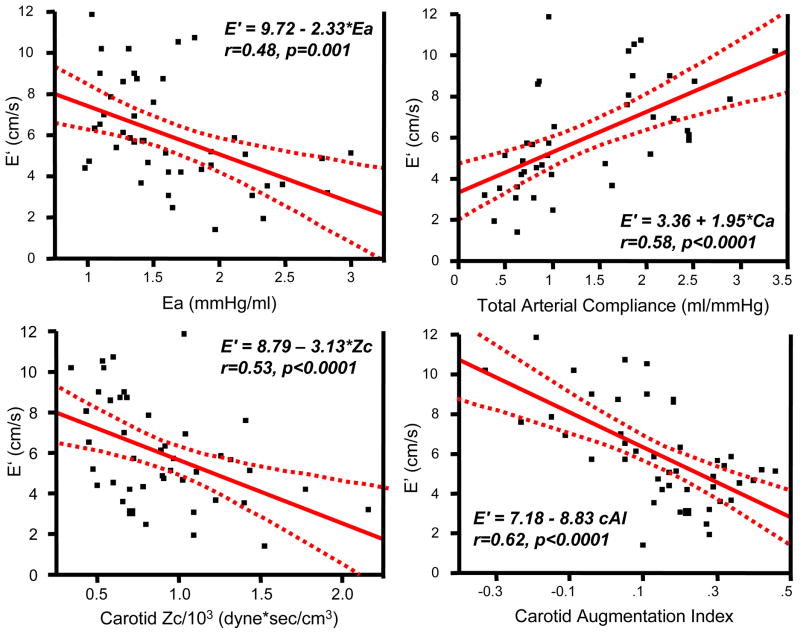
Tissue Doppler-derived early relaxation velocity (E’) varies inversely with afterload and directly with arterial compliance. The relationship between afterload and relaxation is tightest with markers of late systolic load and vascular stiffness (AI, Zc). From Borlaug BA, Melenovsky V, Redfield MM, et al. The impact of arterial load and loading sequence on left ventricular tissue velocities in humans. J Am Coll Card. 2007, in press.
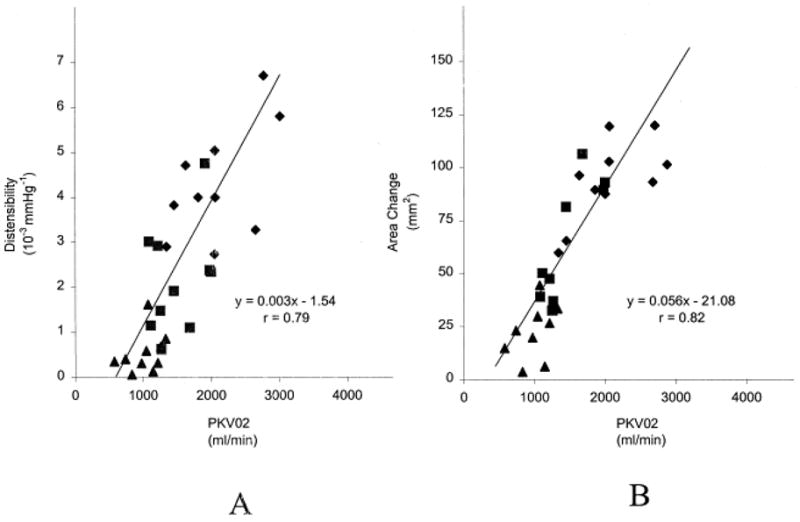
Metabolic exercise performance is directly related to aortic distensibility [A] and cross sectional area change [B] in patients with HFpEF, older-aged controls, and young healthy controls. From Hundley WG, Kitzman DW, Morgan TM, et al. Cardiac cycle-dependent changes in aortic area and distensibility are reduced in older patients with isolated diastolic heart failure and correlate with exercise intolerance. J Am Coll Cardiol. Sep 2001;38(3):796–802
Republished in
-
Ventricular-vascular interaction in heart failure.Cardiol Clin. 2011 Aug;29(3):447-59. doi: 10.1016/j.ccl.2011.06.004. Cardiol Clin. 2011. PMID: 21803232
References
-
- Suga H, Sagawa K. Instantaneous pressure-volume relationships and their ratio in the excised, supported canine left ventricle. Circ Res Jul. 1974;35(1):117–126. - PubMed
-
- Kass DA, Kelly RP. Ventriculo-arterial coupling: concepts, assumptions, and applications. Ann Biomed Eng. 1992;20(1):41–62. - PubMed
-
- Milnor WR. Arterial impedance as ventricular afterload. Circ Res May. 1975;36(5):565–570. - PubMed
-
- Murgo JP, Westerhof N, Giolma JP, Altobelli SA. Aortic input impedance in normal man: relationship to pressure wave forms. Circulation Jul. 1980;62(1):105–116. - PubMed
-
- Sunagawa K, Maughan WL, Burkhoff D, Sagawa K. Left ventricular interaction with arterial load studied in isolated canine ventricle. Am J Physiol Nov. 1983;245(5 Pt 1):H773–780. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
